

Early Noninvasive Detection of Response to Targeted Therapy in Non-Small Cell Lung Cancer
- PMID: 30573519
- PMCID: PMC6481620
- DOI: 10.1158/0008-5472.CAN-18-1082
Early Noninvasive Detection of Response to Targeted Therapy in Non-Small Cell Lung Cancer
Abstract
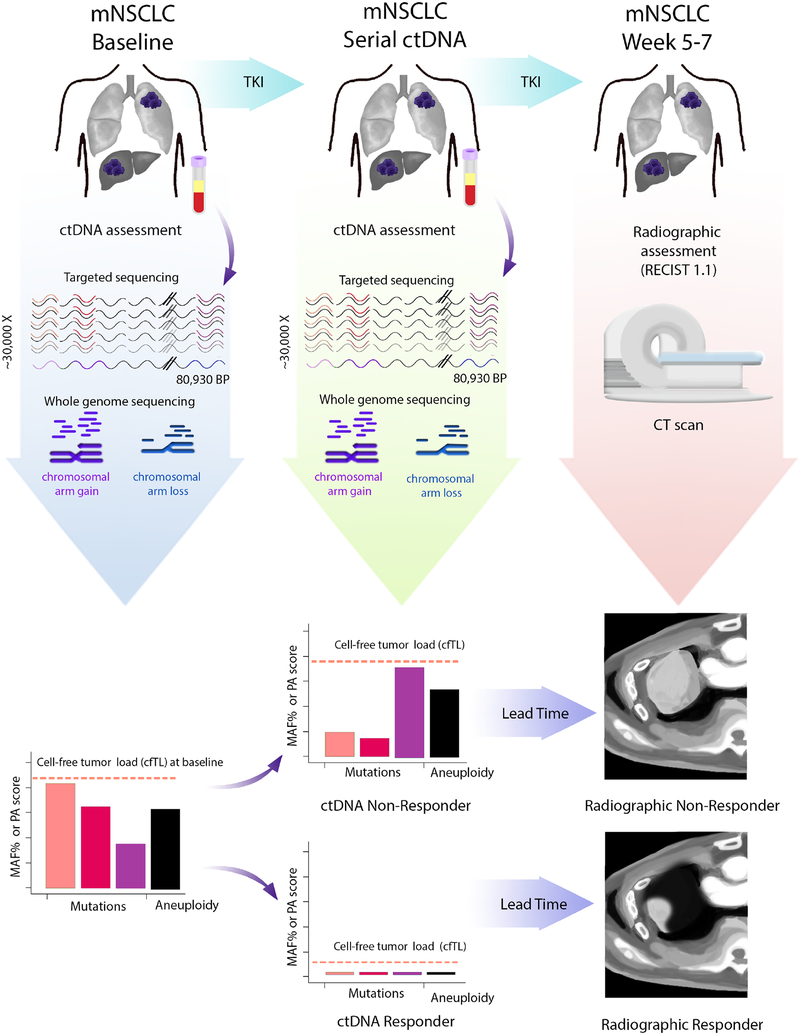
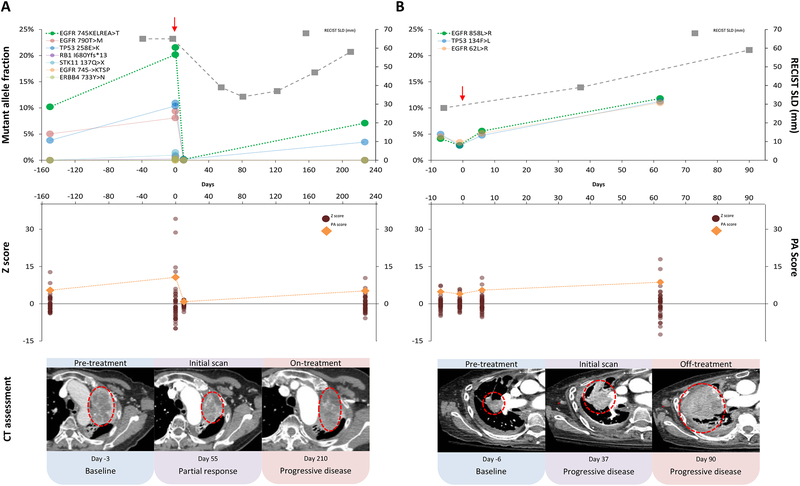
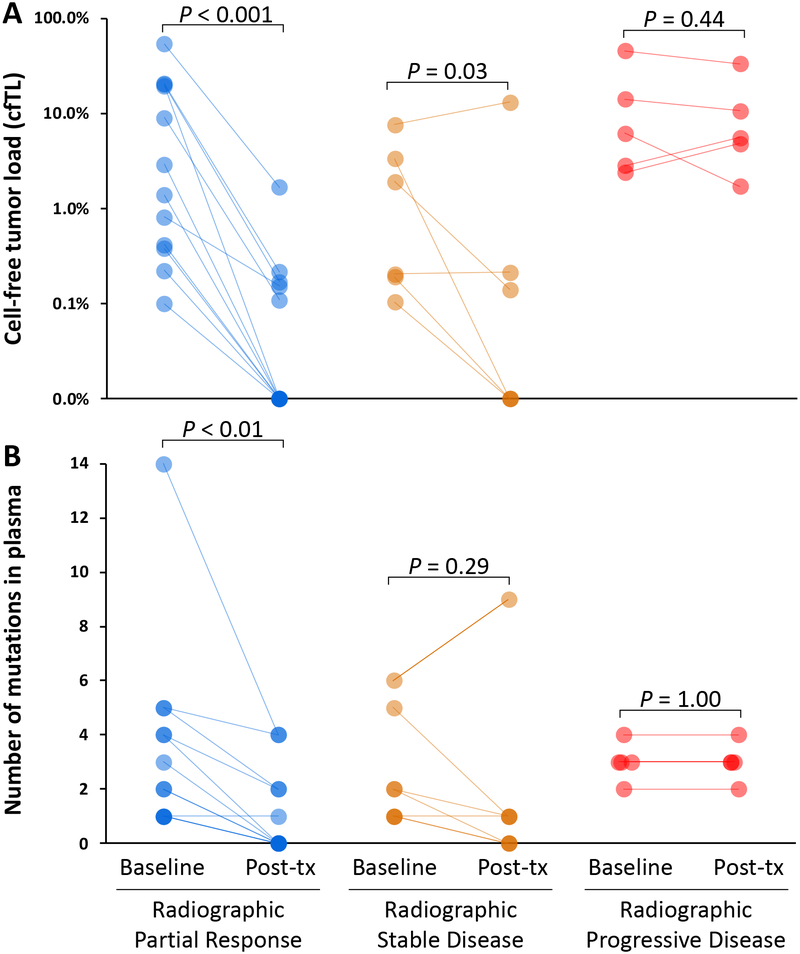
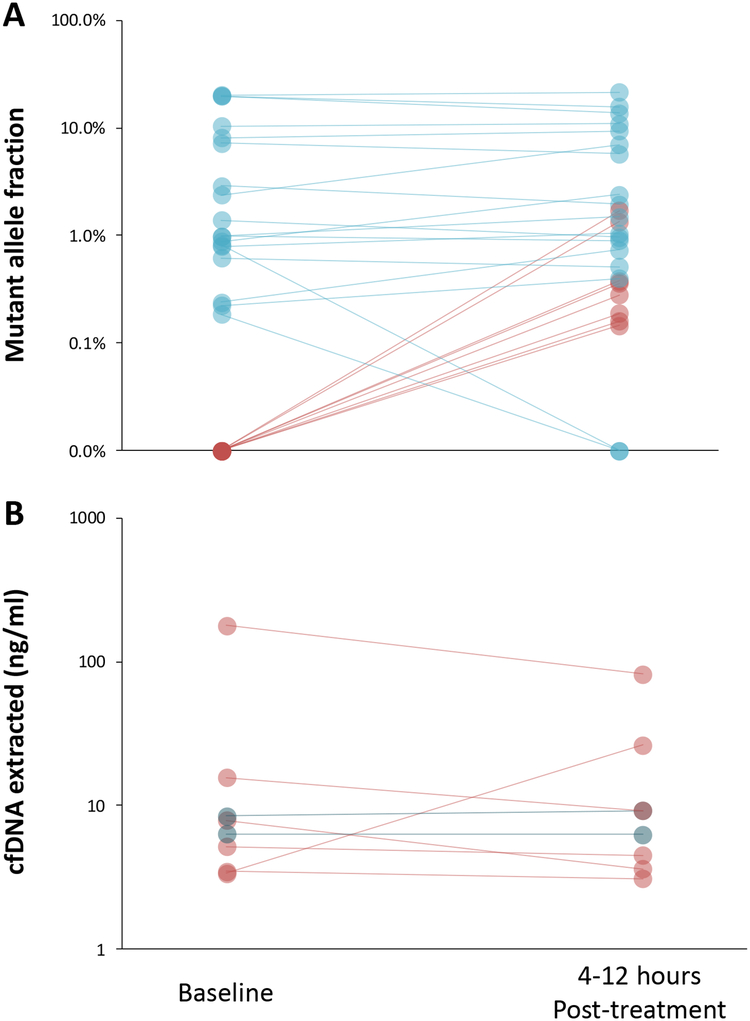
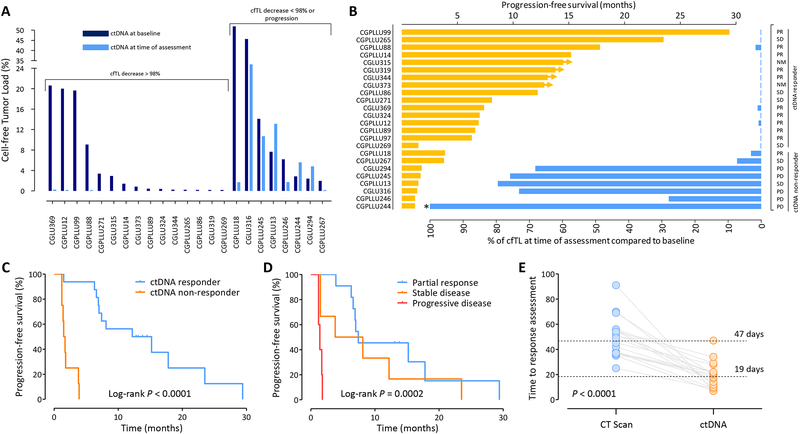
With the advent of precision oncology, there is an urgent need to develop improved methods for rapidly detecting responses to targeted therapies. Here, we have developed an ultrasensitive measure of cell-free tumor load using targeted and whole-genome sequencing approaches to assess responses to tyrosine kinase inhibitors in patients with advanced lung cancer. Analyses of 28 patients treated with anti-EGFR or HER2 therapies revealed a bimodal distribution of cell-free circulating tumor DNA (ctDNA) after therapy initiation, with molecular responders having nearly complete elimination of ctDNA (>98%). Molecular nonresponders displayed limited changes in ctDNA levels posttreatment and experienced significantly shorter progression-free survival (median 1.6 vs. 13.7 months, P < 0.0001; HR = 66.6; 95% confidence interval, 13.0-341.7), which was detected on average 4 weeks earlier than CT imaging. ctDNA analyses of patients with radiographic stable or nonmeasurable disease improved prediction of clinical outcome compared with CT imaging. These analyses provide a rapid approach for evaluating therapeutic response to targeted therapies and have important implications for the management of patients with cancer and the development of new therapeutics.Significance: Cell-free tumor load provides a novel approach for evaluating longitudinal changes in ctDNA during systemic treatment with tyrosine kinase inhibitors and serves an unmet clinical need for real-time, noninvasive detection of tumor response to targeted therapies before radiographic assessment.See related commentary by Zou and Meyerson, p. 1038.
©2018 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
P.M.F. has been a consultant for AstraZeneca/Medimmune and Boehringer-Ingelheim. V. Adleff is a consultant for Personal Genome Diagnostics. V.E.V. is a founder of, holds equity in, and is a member of the Board of Directors of Personal Genome Diagnostics (PGDx). Under a license agreement between PGDx and the Johns Hopkins University, V.E.V. is entitled to a share of royalty received by the University on sales of services or products by PGDx. V.E.V. is a member of the Scientific Advisory Board of Ignyta. The terms of these arrangements have been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. H.H. has served on advisory boards for Astrazeneca, Merck, Boehringer Ingelheim, Abbvie, and Foundation Medicine, speakers honorarium from Bristol Myers Squibb, Merck, and Astrazeneca, and research funding from Pfizer.
Figures
Comment in
-
Circulating Tumor DNA Provides a Sneak Peek into Treatment Responses in Non-Small Cell Lung Cancer.Cancer Res. 2019 Mar 15;79(6):1038-1040. doi: 10.1158/0008-5472.CAN-19-0231. Cancer Res. 2019. PMID: 30877100 Free PMC article.
References
-
- Sawyers C Targeted cancer therapy. Nature 2004;432:294–7 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
