

Unexpected Fat Distribution in Adolescents With Narcolepsy
- PMID: 30574118
- PMCID: PMC6292486
- DOI: 10.3389/fendo.2018.00728
Unexpected Fat Distribution in Adolescents With Narcolepsy
Abstract
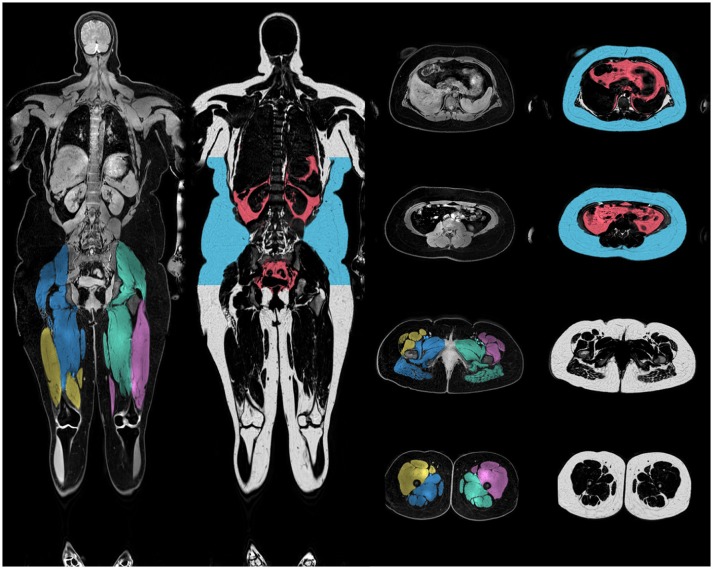
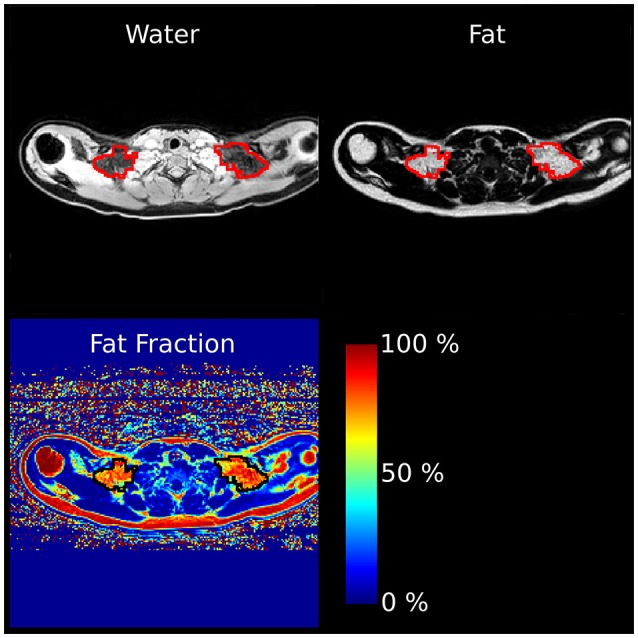
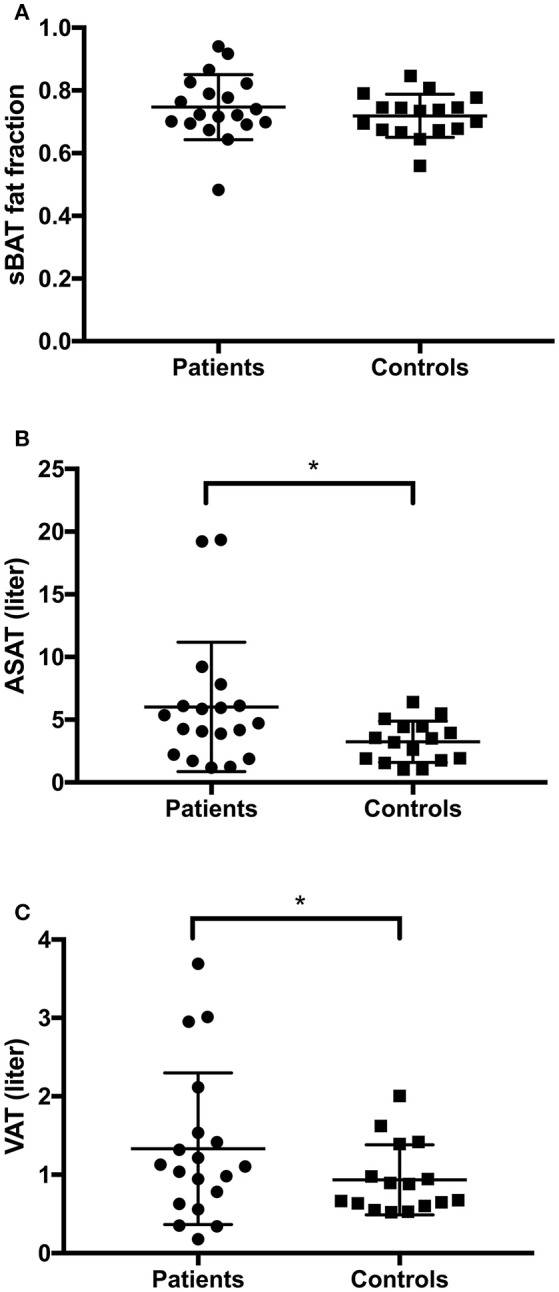
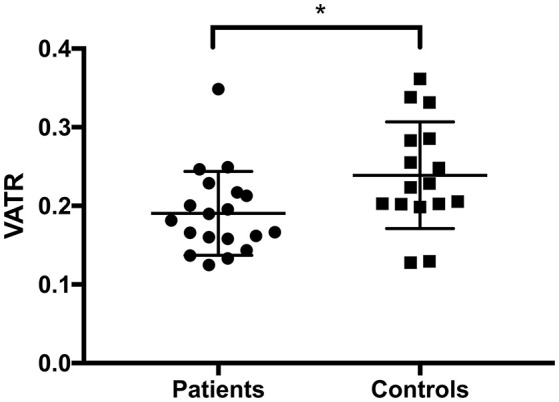
Narcolepsy type 1 is a chronic sleep disorder with significantly higher BMI reported in more than 50% of adolescent patients, putting them at a higher risk for metabolic syndrome in adulthood. Although well-documented, the body fat distribution and mechanisms behind weight gain in narcolepsy are still not fully understood but may be related to the loss of orexin associated with the disease. Orexin has been linked to the regulation of brown adipose tissue (BAT), a metabolically active fat involved in energy homeostasis. Previous studies have used BMI and waist circumference to characterize adipose tissue increases in narcolepsy but none have investigated its specific distribution. Here, we examine adipose tissue distribution in 19 adolescent patients with narcolepsy type 1 and compare them to 17 of their healthy peers using full body magnetic resonance imaging (MRI). In line with previous findings we saw that the narcolepsy patients had more overall fat than the healthy controls, but contrary to our expectations there were no group differences in supraclavicular BAT, suggesting that orexin may have no effect at all on BAT, at least under thermoneutral conditions. Also, in line with previous reports, we observed that patients had more total abdominal adipose tissue (TAAT), however, we found that they had a lower ratio between visceral adipose tissue (VAT) and TAAT indicating a relative increase of subcutaneous abdominal adipose tissue (ASAT). This relationship between VAT and ASAT has been associated with a lower risk for metabolic disease. We conclude that while weight gain in adolescents with narcolepsy matches that of central obesity, the lower VAT ratio may suggest a lower risk of developing metabolic disease.
Keywords: BMI; brown adipose tissue; hypocretin; magnetic resonance imaging (MRI); obesity; orexin; subcutaneous adipose tissue; visceral adipose tissue.
Figures
Similar articles
-
Role of Brown Adipose Tissue in Adiposity Associated With Narcolepsy Type 1.Front Endocrinol (Lausanne). 2020 Apr 16;11:145. doi: 10.3389/fendo.2020.00145. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32373062 Free PMC article. Review.
-
Correlation of fat distribution in whole body MRI with generally used anthropometric data.Invest Radiol. 2009 Nov;44(11):712-9. doi: 10.1097/RLI.0b013e3181afbb1e. Invest Radiol. 2009. PMID: 19809346
-
Correlation of Brown Adipose Tissue with Other Body Fat Compartments and Patient Characteristics: A Retrospective Analysis in a Large Patient Cohort Using PET/CT.Acad Radiol. 2018 Jan;25(1):102-110. doi: 10.1016/j.acra.2017.09.007. Epub 2017 Nov 3. Acad Radiol. 2018. PMID: 29108812
-
Subtraction of subcutaneous fat to improve the prediction of visceral adiposity: exploring a new anthropometric track in overweight and obese youth.Pediatr Diabetes. 2017 Aug;18(5):399-404. doi: 10.1111/pedi.12415. Epub 2016 Jul 12. Pediatr Diabetes. 2017. PMID: 27400675
-
Depot-specific hormonal characteristics of subcutaneous and visceral adipose tissue and their relation to the metabolic syndrome.Horm Metab Res. 2002 Nov-Dec;34(11-12):616-21. doi: 10.1055/s-2002-38256. Horm Metab Res. 2002. PMID: 12660870 Review.
Cited by
-
Role of Brown Adipose Tissue in Adiposity Associated With Narcolepsy Type 1.Front Endocrinol (Lausanne). 2020 Apr 16;11:145. doi: 10.3389/fendo.2020.00145. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32373062 Free PMC article. Review.
-
Metabolic signals in sleep regulation: the role of brown adipose tissue.Neurobiol Sleep Circadian Rhythms. 2025 Apr 24;18(Suppl):100122. doi: 10.1016/j.nbscr.2025.100122. eCollection 2025 May. Neurobiol Sleep Circadian Rhythms. 2025. PMID: 40703579 Free PMC article.
-
Associations of plasma hypocretin-1 with metabolic and reproductive health: Two systematic reviews of clinical studies.Sleep Med Rev. 2020 Aug;52:101307. doi: 10.1016/j.smrv.2020.101307. Epub 2020 Mar 17. Sleep Med Rev. 2020. PMID: 32259696 Free PMC article.
-
Orexins/Hypocretins: Key Regulators of Energy Homeostasis.Front Endocrinol (Lausanne). 2019 Dec 10;10:830. doi: 10.3389/fendo.2019.00830. eCollection 2019. Front Endocrinol (Lausanne). 2019. PMID: 31920958 Free PMC article. Review.
-
Body Weight and Metabolic Rate Changes in Narcolepsy: Current Knowledge and Future Directions.Metabolites. 2022 Nov 16;12(11):1120. doi: 10.3390/metabo12111120. Metabolites. 2022. PMID: 36422261 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources