

Risks for lymphoma and gastrointestinal carcinoma in patients with newly diagnosed adult-onset celiac disease: Consequences for follow-up: Celiac disease, lymphoma and GI carcinoma
- PMID: 30574319
- PMCID: PMC6297918
- DOI: 10.1177/2050640618800540
Risks for lymphoma and gastrointestinal carcinoma in patients with newly diagnosed adult-onset celiac disease: Consequences for follow-up: Celiac disease, lymphoma and GI carcinoma
Abstract
Background: The association between celiac disease (CD) and the development of lymphoid and gastrointestinal (GI) malignancies have been reported. However, data are scarce yet needed to develop evidence-based follow-up programs.
Objective: The objective of this article is to assess relative (RR) and absolute risks of lymphoma and GI carcinoma for newly diagnosed patients.
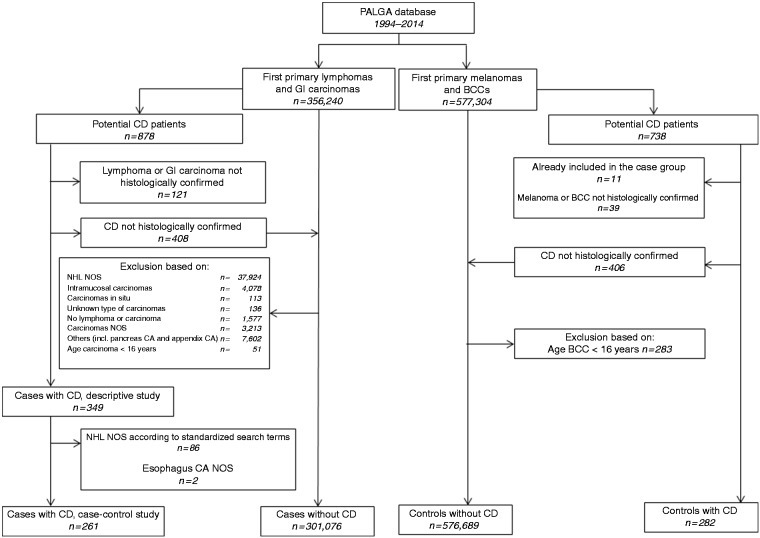
Methods: A case-control design to determine RR was performed with cases (lymphoma or GI carcinoma) and controls (melanoma or basal cell carcinoma) diagnosed 1994-2014, retrieved from the Dutch nationwide population-based pathology database (PALGA). Within this population, individuals with histologically proven CD before or simultaneously diagnosed with the malignancy were identified.
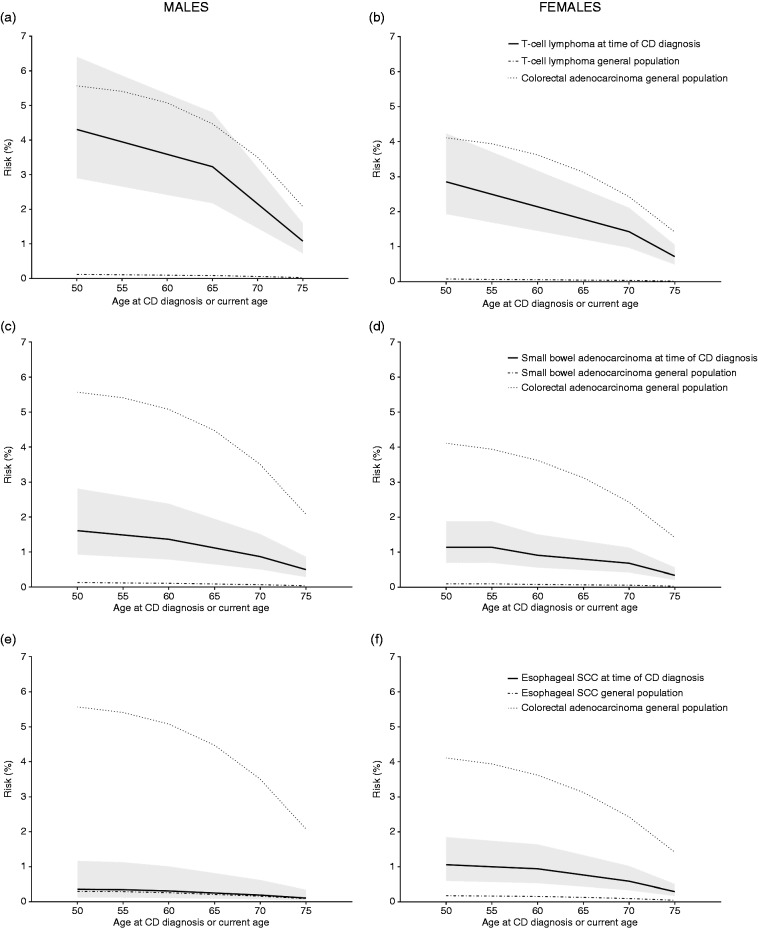
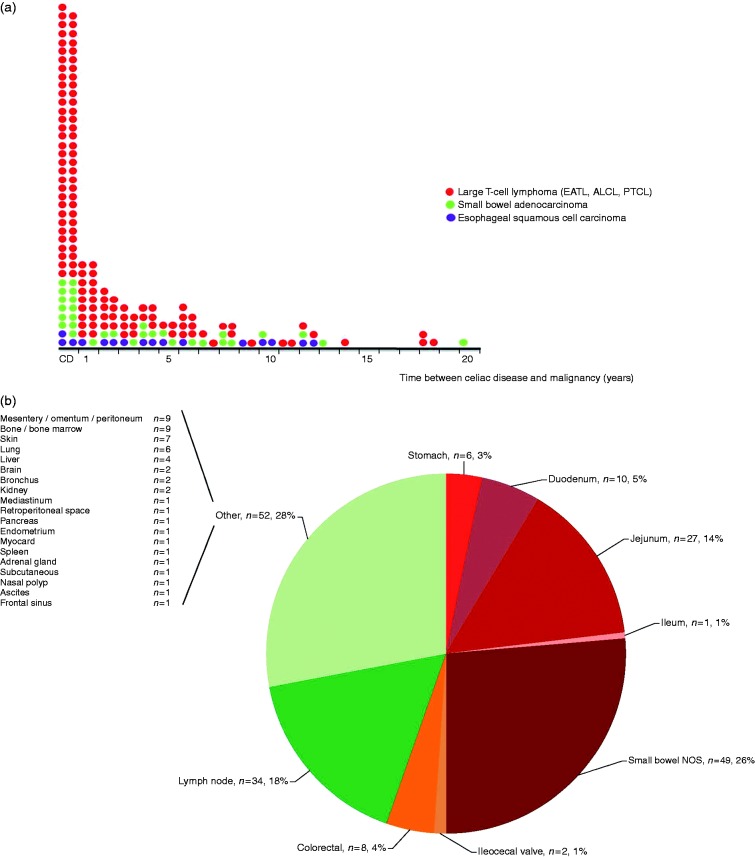
Results: A total of 349/301,425 cases (0.1%) and 282/576,971 (0.05%) controls were diagnosed with CD. Risk of T-cell lymphoma, predominantly enteropathy-associated T-cell lymphoma (EATL), was strongly associated with CD diagnosis (RR = 35.8 (95% CI 27.1-47.4)). Although most often synchronously diagnosed, T-cell lymphoma RR ≥ 1 year after CD diagnosis was still elevated (RR = 12.7 (95% CI 7.6-21.3)). Other CD-associated malignancies were small bowel adenocarcinoma (RR = 11.9 (95% CI 8.2-17.2)) and esophageal squamous cell carcinoma (RR = 3.5 (95% CI 2.1-5.8)). Absolute risks were relatively low. Other types of lymphomas and GI carcinomas were not associated with CD.
Conclusion: Increased risk for specific malignancies in CD should alert physicians for EATL (both intestinal and extraintestinal) and small bowel adenocarcinoma in patients with CD diagnosed at age ≥ 50 years.
Keywords: Celiac disease; enteropathy-associated T-cell lymphoma; follow-up; small bowel adenocarcinoma; squamous cell carcinoma.
Figures
References
-
- Green PH, Cellier C. Celiac disease. N Engl J Med 2007; 357: 1731–1743. - PubMed
-
- Aparicio T, Zaanan A, Svrcek M, et al. Small bowel adenocarcinoma: Epidemiology, risk factors, diagnosis and treatment. Dig Liver Dis 2014; 46: 97–104. - PubMed
-
- Verbeek WH, Van De Water JM, Al-Toma A, et al. Incidence of enteropathy-associated T-cell lymphoma: A nation-wide study of a population-based registry in The Netherlands. Scand J Gastroenterol 2008; 43: 1322–1328. - PubMed
-
- Ilus T, Kaukinen K, Virta LJ, et al. Incidence of malignancies in diagnosed celiac patients: A population-based estimate. Am J Gastroenterol 2014; 109: 1471–1477. - PubMed
LinkOut - more resources
Full Text Sources
