

Presentation and Outcomes After Medical and Surgical Treatment Versus Medical Treatment Alone of Spontaneous Infectious Spondylodiscitis: A Systematic Literature Review and Meta-Analysis
- PMID: 30574438
- PMCID: PMC6295820
- DOI: 10.1177/2192568218799058
Presentation and Outcomes After Medical and Surgical Treatment Versus Medical Treatment Alone of Spontaneous Infectious Spondylodiscitis: A Systematic Literature Review and Meta-Analysis
Abstract
Study design: Systematic literature review.
Objectives: The aims of this study were to (1) describe the clinical features, disabilities, and incidence of neurologic deficits of pyogenic spondylodiscitis prior to treatment and (2) compare the functional outcomes between patients who underwent medical treatment alone or in combination with surgery for pyogenic spondylodiscitis.
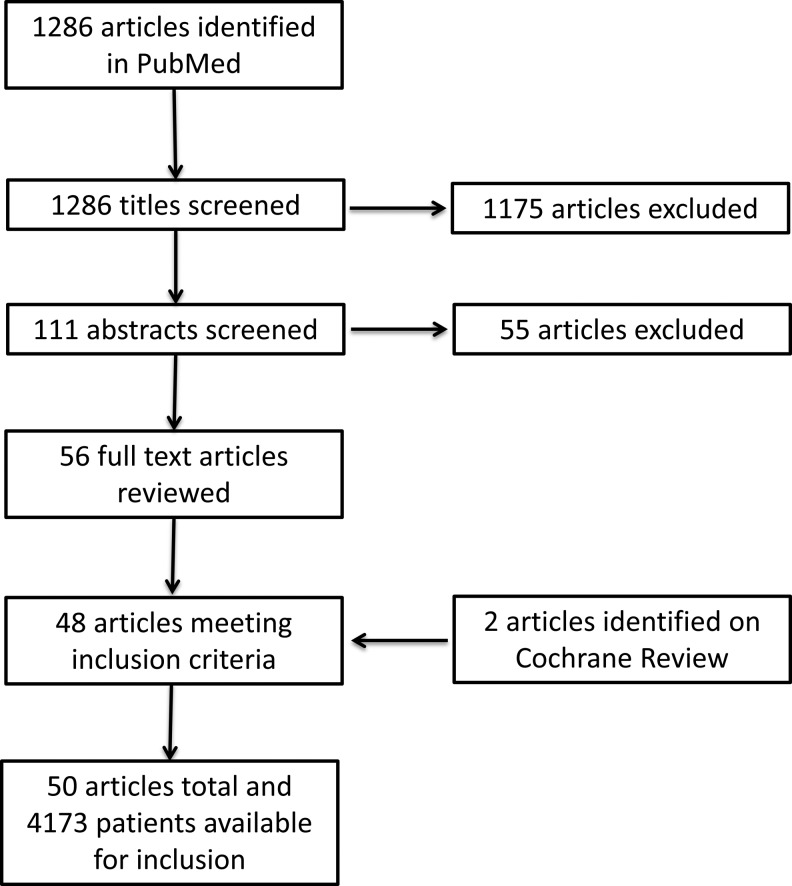
Methods: A systematic literature review was performed using PubMed according to PRISMA guidelines. No year restriction was put in place. Statistical analysis of pooled data, when documented in the original report (ie, number of patients with desired variable and number of patients evaluated), was conducted to determine the most common presenting symptoms, incidence of pre- and postoperative neurologic deficits, associated comorbidities, infectious pathogens, approach for surgery when performed, and duration of hospitalization. Outcomes data, including return to work status, resolution of back pain, and functional recovery were also pooled among all studies and surgery-specific studies alone. Meta-analysis of studies with subgroup analysis of pain-free outcome in surgical and medical patients was performed.
Results: Fifty of 1286 studies were included, comprising 4173 patients undergoing either medical treatment alone or in combination with surgery. Back pain was the most common presenting symptom, reported in 91% of patients. Neurologic deficit was noted in 31% of patients. Staphylococcus aureus was the most commonly reported pathogen, seen in 35% of reported cases. Decompression and fusion was the most commonly reported surgical procedure, performed in 80% of the surgically treated patients. Combined anterior-posterior procedures and staged surgeries were performed in 33% and 26% of surgeries, respectively. The meta-analysis comparing visual analog scale score at follow-up was superior among patients receiving surgery over medical treatment alone (mean difference -0.61, CI -0.90 to -0.25), while meta-analysis comparing freedom from pain in patients receiving medical treatment alone versus combined medical and surgical treatment demonstrated superior pain-free outcomes among surgical series (odds ratio 5.35, CI 2.27-12.60, P < .001), but was subject to heterogeneity among studies (I 2 = 56%, P = .13). Among all patients, freedom from pain was achieved in 79% of patients, and an excellent outcome was achieved in 73% of patients.
Conclusion: Medical management remains first-line treatment of infectious pyogenic spondylodiscitis. Surgery may be indicated for progressive pain, persistent infection on imaging, deformity or neurologic deficits. If surgery is required, reported literature shows potential for significant pain reduction, improved neurologic function and a high number of patients returning to a normal functional/work status.
Keywords: back pain; discitis; osteodiscitis; outcome; pyogenic; spondylodiscitis.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James Harrop, MD, receives speaking honorarium from Globus and is a consultant for Ethicon. Christopher I. Shaffrey, MD, is a consultant for Medtronic, Nuvasive, Zimmer Biomet, K2M, Stryker, and In Vivo; receives royalties from Medtronic, Nuvasive, and Zimmer Biomet; has patents with Medtronic, Nuvasive, and Zimmer Biomet; is a stockholder in Nuvasive; and receives grants from the NIH, Department of Defense, ISSG, DePuy Synthes, and AO. Justin S. Smith, MD, PhD, is a consultant for Zimmer Biomet, Nuvasive, K2M, Allsource and a past consultant for Cerapedics; receives honorarium for teaching from Zimmer Biomet, Nuvasive, and K2M; receives royalties from Zimmer Biomet; receives research study group support from DePuy Synthes/ISSG; and receives fellowship funding from NREF and AOSpine.
Figures


References
-
- Zimmerli W. Clinical practice. Vertebral osteomyelitis. N Engl J Med. 2010;362:1022–1029. - PubMed
-
- Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008;56:401–412. - PubMed
-
- Lu ML, Niu CC, Tsai TT, Fu TS, Chen LH, Chen WJ. Transforaminal lumbar interbody debridement and fusion for the treatment of infective spondylodiscitis in the lumbar spine. Eur Spine J. 2015;24:555–560. - PubMed
-
- Batirel A, Erdem H, Sengoz G, et al. The course of spinal tuberculosis (Pott disease): results of the multinational, multicentre Backbone-2 study. Clin Microbiol Infect. 2015;21:1008e9–1008.e18. - PubMed
-
- Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62:1006–1012. - PubMed
LinkOut - more resources
Full Text Sources
