

Intra- and interreader reproducibility of PI-RADSv2: A multireader study
- PMID: 30575184
- PMCID: PMC6504619
- DOI: 10.1002/jmri.26555
Intra- and interreader reproducibility of PI-RADSv2: A multireader study
Abstract
Background: The Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) has been in use since 2015; while interreader reproducibility has been studied, there has been a paucity of studies investigating the intrareader reproducibility of PI-RADSv2.
Purpose: To evaluate both intra- and interreader reproducibility of PI-RADSv2 in the assessment of intraprostatic lesions using multiparametric magnetic resonance imaging (mpMRI).
Study type: Retrospective.
Population/subjects: In all, 102 consecutive biopsy-naïve patients who underwent prostate MRI and subsequent MR/transrectal ultrasonography (MR/TRUS)-guided biopsy.
Field strength/sequences: Prostate mpMRI at 3T using endorectal with phased array surface coils (TW MRI, DW MRI with ADC maps and b2000 DW MRI, DCE MRI).
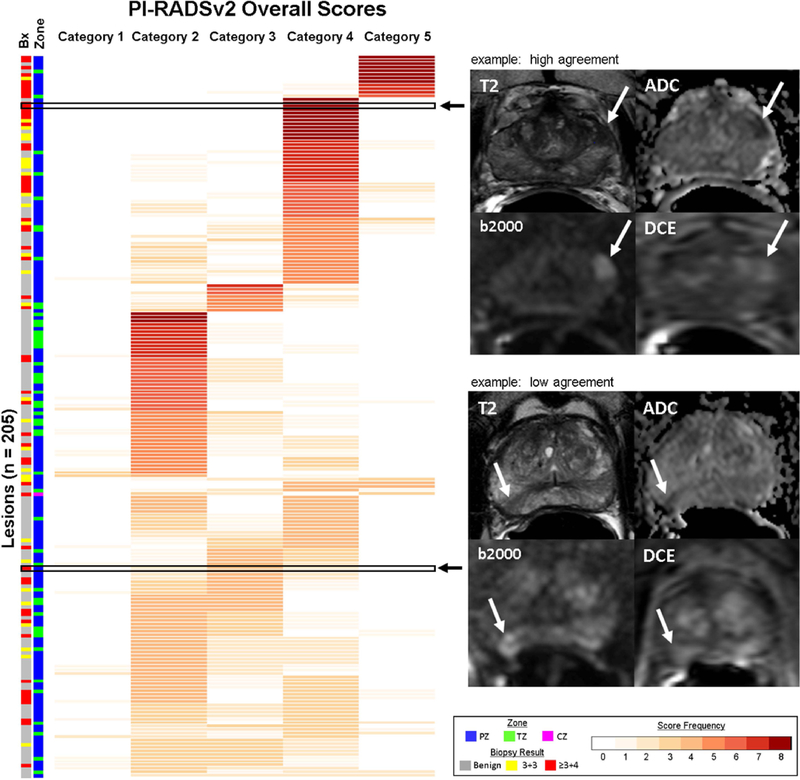
Assessment: Previously detected and biopsied lesions were scored by four readers from four different institutions using PI-RADSv2. Readers scored lesions during two readout rounds with a 4-week washout period.
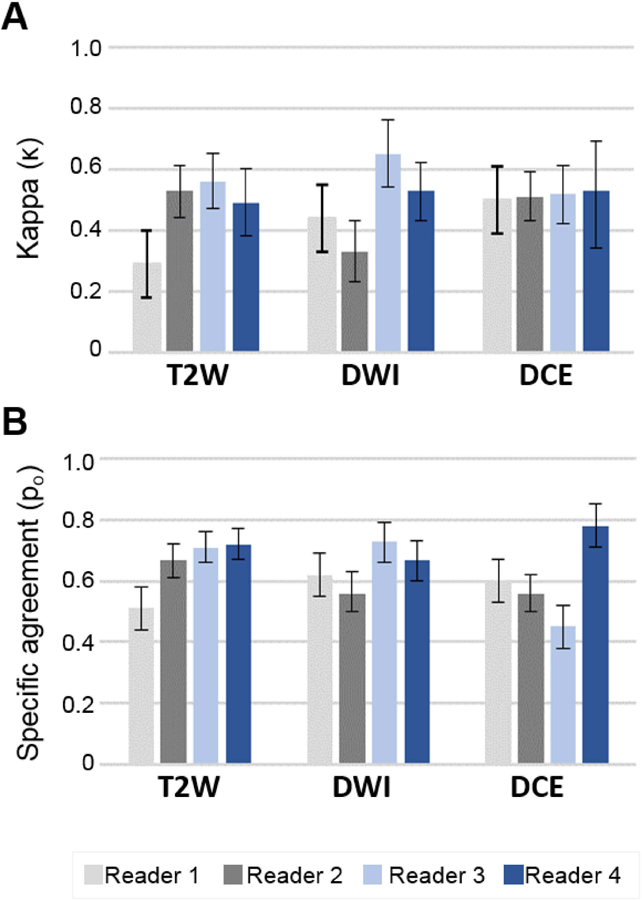
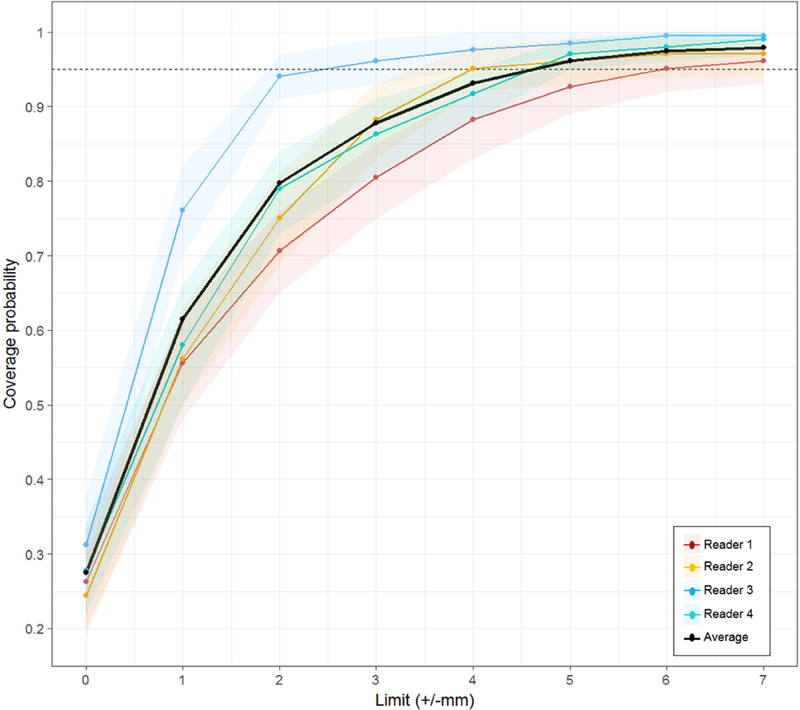
Statistical tests: Kappa (κ) statistics and specific agreement (Po ) were calculated to quantify intra- and interreader reproducibility of PI-RADSv2 scoring. Lesion measurement agreement was calculated using the intraclass correlation coefficient (ICC).
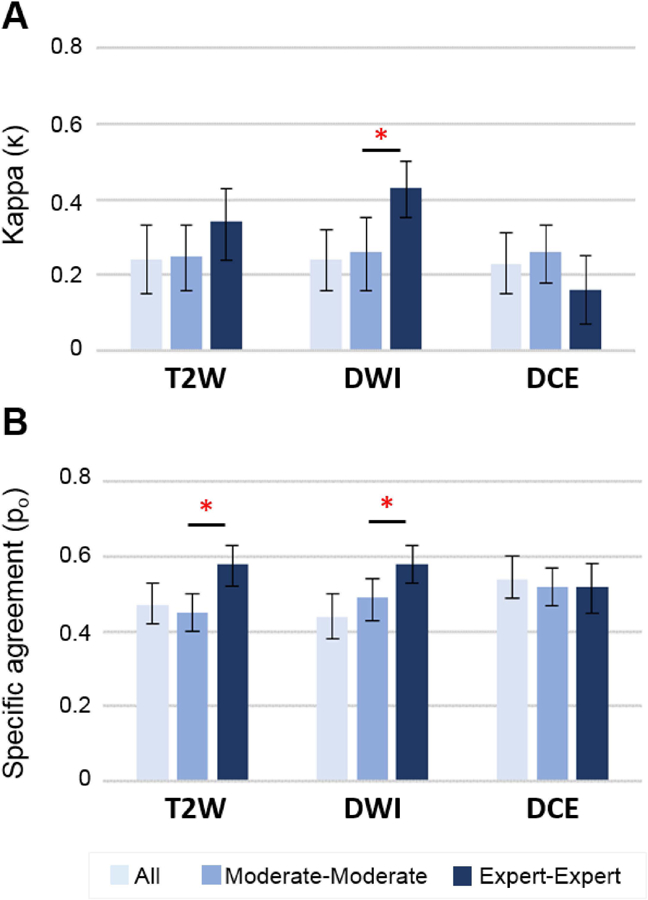
Results: Overall intrareader reproducibility was moderate to substantial (κ = 0.43-0.67, Po = 0.60-0.77), while overall interreader reproducibility was poor to moderate (κ = 0.24, Po = 46). Readers with more experience showed greater interreader reproducibility than readers with intermediate experience in the whole prostate (P = 0.026) and peripheral zone (P = 0.002). Sequence-specific interreader agreement for all readers was similar to the overall PI-RADSv2 score, with κ = 0.24, 0.24, and 0.23 and Po = 0.47, 0.44, and 0.54 in T2 -weighted, diffusion-weighted imaging (DWI), and dynamic contrast-enhanced (DCE), respectively. Overall intrareader and interreader ICC for lesion measurement was 0.82 and 0.71, respectively.
Data conclusion: PI-RADSv2 provides moderate intrareader reproducibility, poor interreader reproducibility, and moderate interreader lesion measurement reproducibility. These findings suggest a need for more standardized reader training in prostate MRI.
Level of evidence: 2 Technical Efficacy: Stage 2.
Keywords: MRI; PI-RADS; prostate cancer; reader reproducibility.
© 2018 International Society for Magnetic Resonance in Medicine.
Conflict of interest statement
Conflict of Interest:
Author BJW is supported by the Intramural Research Program of the NIH and the NIH Center for Interventional Oncology and NIH Grant # Z1A CL040015–08. NIH and Philips / InVivo Inc have a cooperative Research and Development Agreement. NIH and Philips / InVivo Inc have a patent license agreement and NIH and BJW, BT, PAP, PLC may receive royalties. The remaining authors have no disclosures.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
