

Dormancy in cancer
- PMID: 30575231
- PMCID: PMC6361606
- DOI: 10.1111/cas.13917
Dormancy in cancer
Abstract
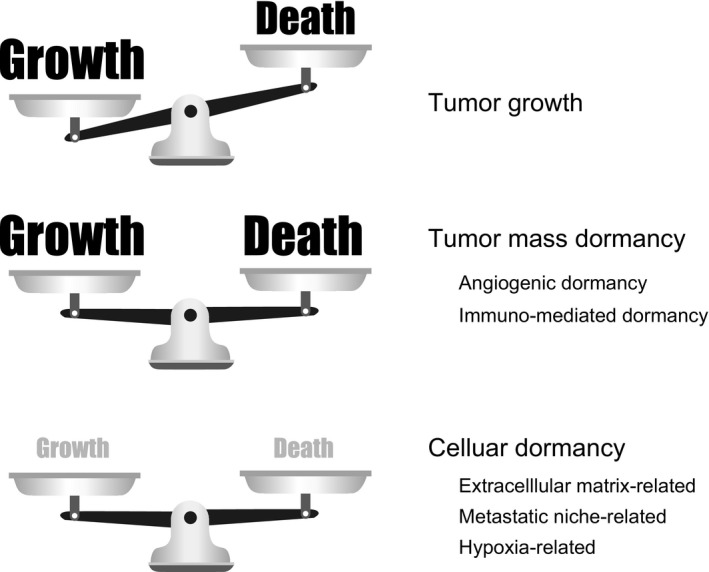
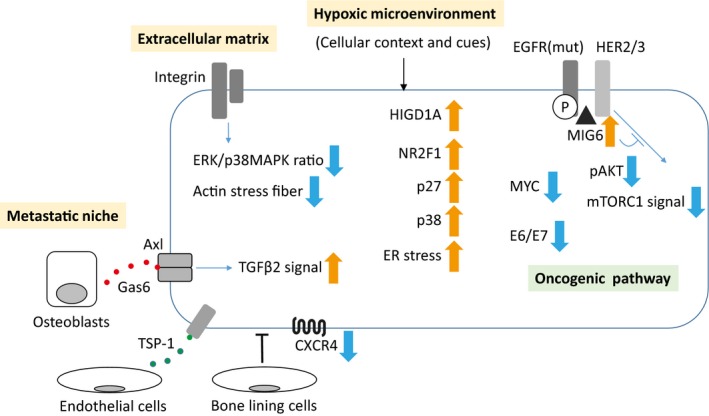
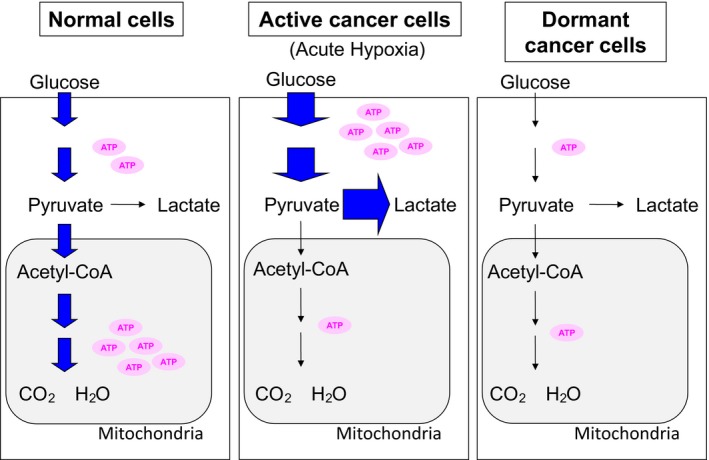
The idea of tumor dormancy originated from clinical findings that recurrence of cancer occurs several years or even several decades after surgical resection of the primary tumor. Tumor mass dormancy was proposed as a model, where there is equal balance between increases in the number of cancer cells by proliferation and decreases as a result of cell death. Tumor mass dormancy includes angiogenic dormancy and immune-mediated dormancy. Another emerging type of tumor dormancy is cellular dormancy in which cancer cells are in a quiescent state. Cellular dormancy is induced by cues such as the extracellular matrix environment, metastatic niches, a hypoxic microenvironment, and endoplasmic reticulum stress. Even the oncogenic pathways, on which active cancer cells depend for survival and growth, are suppressed in the dormant state. As tumor dormancy is one of the mechanisms of resistance against various cancer therapies, targeting dormant cancer cells should be considered for future treatment strategies.
© 2018 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Figures
References
-
- Weckermann D, Muller P, Wawroschek F, Harzmann R, Riethmuller G, Schlimok G. Disseminated cytokeratin positive tumor cells in the bone marrow of patients with prostate cancer: detection and prognostic value. J Urol. 2001;166:699‐703. - PubMed
-
- Dent R, Trudeau M, Pritchard KI, et al. Triple‐negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429‐4434. - PubMed
-
- Romero A, Prat A, Garcia‐Saenz JA, et al. Assignment of tumor subtype by genomic testing and pathologic‐based approximations: implications on patient's management and therapy selection. Clin Transl Oncol. 2014;16:386‐394. - PubMed
-
- Prat A, Pineda E, Adamo B, et al. Clinical implications of the intrinsic molecular subtypes of breast cancer. Breast. 2015;24(Suppl 2):S26‐S35. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
