

Clinical practice guidelines for IgG4-related sclerosing cholangitis
- PMID: 30575336
- PMCID: PMC6590186
- DOI: 10.1002/jhbp.596
Clinical practice guidelines for IgG4-related sclerosing cholangitis
Abstract
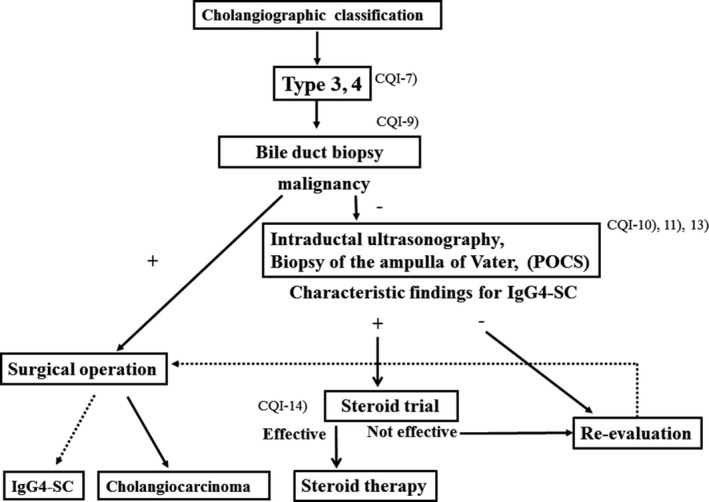
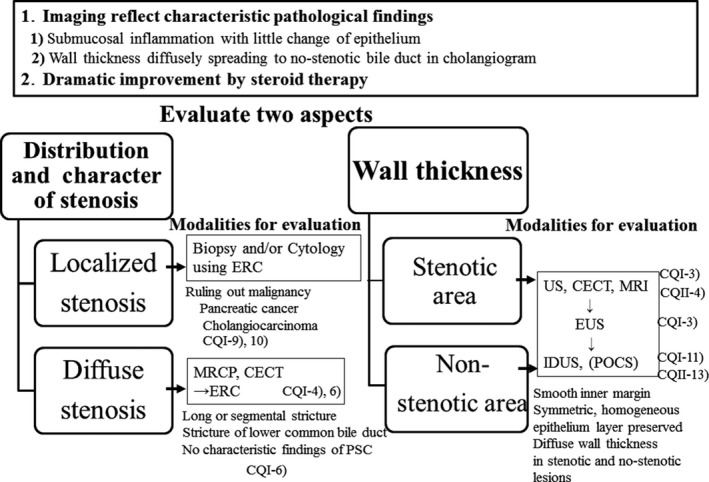
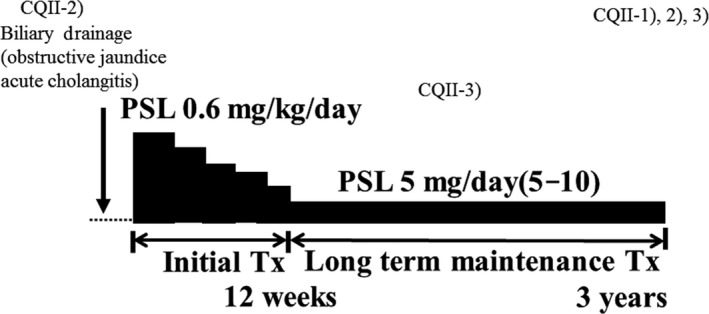
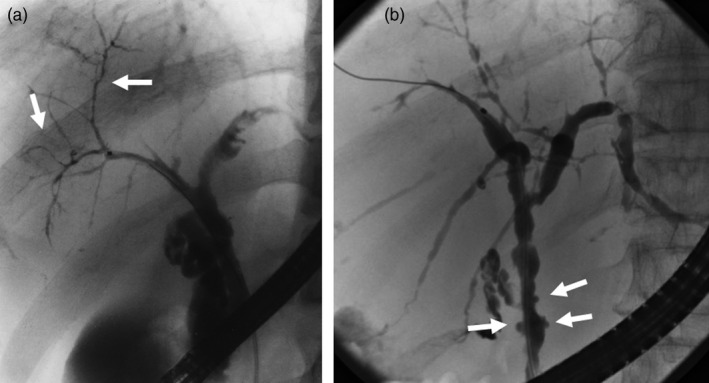
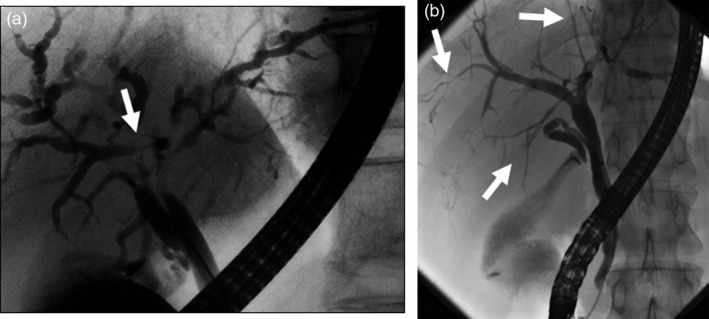
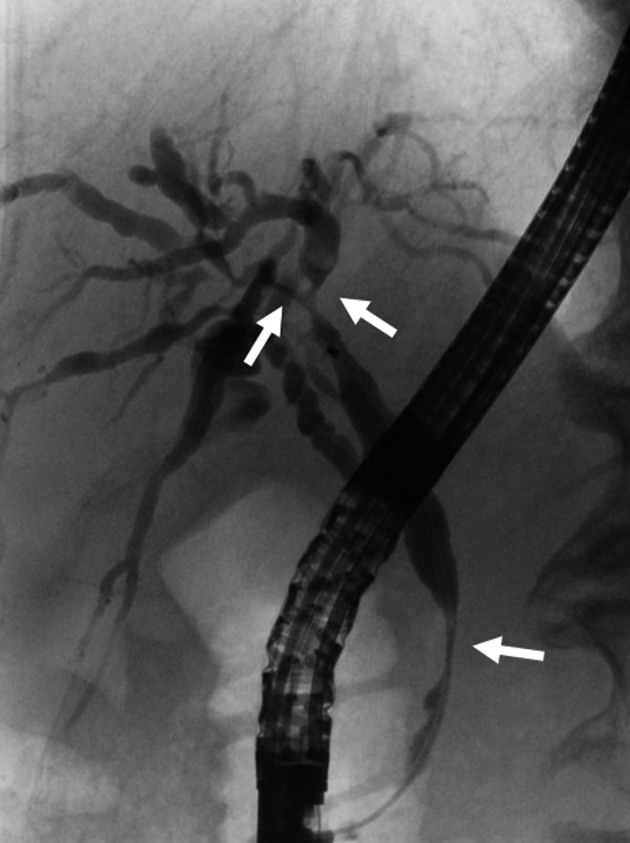
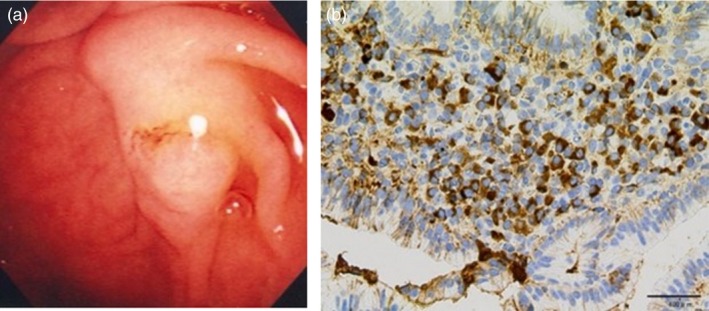
IgG4-related sclerosing cholangitis (IgG4-SC) is a distinct type of cholangitis frequently associated with autoimmune pancreatitis and currently recognized as a biliary manifestation of IgG4-related disease. Although clinical diagnostic criteria of IgG4-SC were established in 2012, differential diagnosis from primary sclerosing cholangitis and cholangiocarcinoma is sometimes difficult. Furthermore, no practical guidelines for IgG4-SC are available. Because the evidence level of most articles retrieved through searching the PubMed, Cochrane Library, and Igaku Chuo Zasshi databases was below C based on the systematic review evaluation system of clinical practice guidelines MINDS 2014, we developed consensus guidelines using the modified Delphi approach. Three committees (a guideline creating committee, an expert panelist committee for rating statements according to the modified Delphi method, and an evaluating committee) were organized. Eighteen clinical questions (CQs) with clinical statements were developed regarding diagnosis (14 CQs) and treatment (4 CQs). Recommendation levels for clinical statements were set using the modified Delphi approach. The guidelines explain methods for accurate diagnosis, and safe and appropriate treatment of IgG4-SC.
Keywords: Bile duct; Guideline; IgG4; Sclerosing cholangitis; Steroid.
© 2018 The Authors. Journal of Hepato-Biliary-Pancreatic Sciences published by John Wiley & Sons Australia, Ltd on behalf of Japanese Society of Hepato-Biliary-Pancreatic Surgery.
Conflict of interest statement
None declared.
Figures


References
-
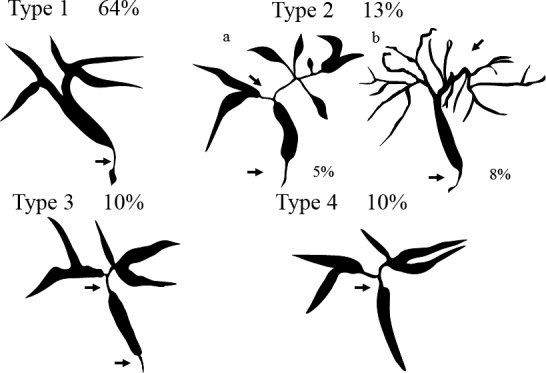
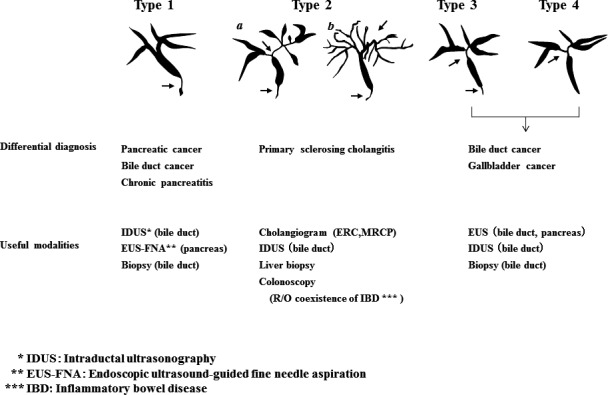
- Nakazawa T, Naitoh I, Hayashi K, Okumura F, Miyabe K, Yoshida M, et al. Diagnostic criteria for IgG4‐related sclerosing cholangitis based on cholangiographic classification. J Gastroenterol 2012;47:79–87. - PubMed
-
- Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4‐related disease. Lancet. 2015;385:1460–71. - PubMed
-
- Ohara H, Okazaki K, Tsubouchi H, Inui K, Kawa S, Kamisawa T, et al. Clinical diagnostic criteria of IgG4‐related sclerosing cholangitis 2012. J Hepatobiliary Pancreat Sci. 2012;19:536–42. - PubMed
-
- Minds Guideline Center , Japan Council for Quality Health Care. Minds handbook for clinical practice guideline development 2014. 2014. Available from URL: https://minds.jcqhc.or.jp/s/guidance
-
- Fitch K, Bernstein SJ, Aguilar MS. The RAND/UCLA appropriateness method user's manual. Santa Monica: RAND; 2001.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
