

Association of Scheduled vs Emergency-Only Dialysis With Health Outcomes and Costs in Undocumented Immigrants With End-stage Renal Disease
- PMID: 30575859
- PMCID: PMC6439652
- DOI: 10.1001/jamainternmed.2018.5866
Association of Scheduled vs Emergency-Only Dialysis With Health Outcomes and Costs in Undocumented Immigrants With End-stage Renal Disease
Abstract
Importance: In 40 of 50 US states, scheduled dialysis is withheld from undocumented immigrants with end-stage renal disease (ESRD); instead, they receive intermittent emergency-only dialysis to treat life-threatening manifestations of ESRD. However, the comparative effectiveness of scheduled dialysis vs emergency-only dialysis and the influence of treatment on health outcomes, utilization, and costs is uncertain.
Objective: To compare the effectiveness of scheduled vs emergency-only dialysis with regard to health outcomes, utilization, and costs in undocumented immigrants with ESRD.
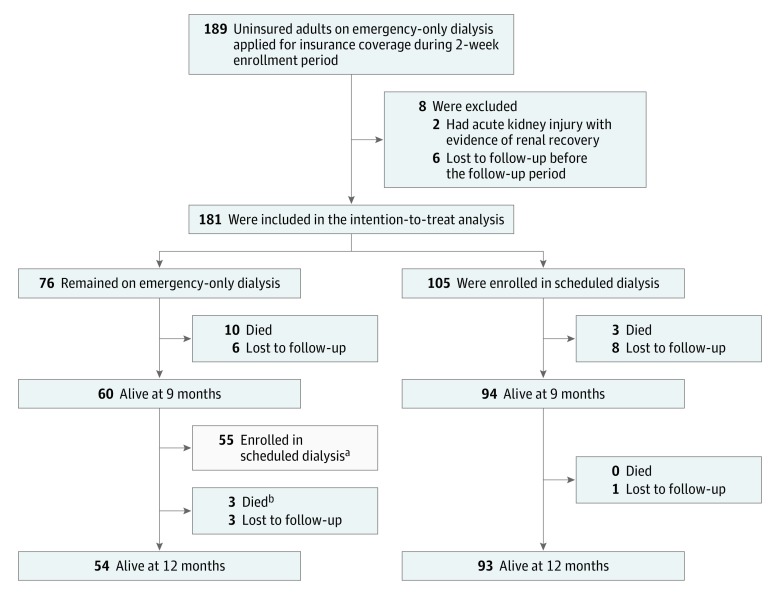
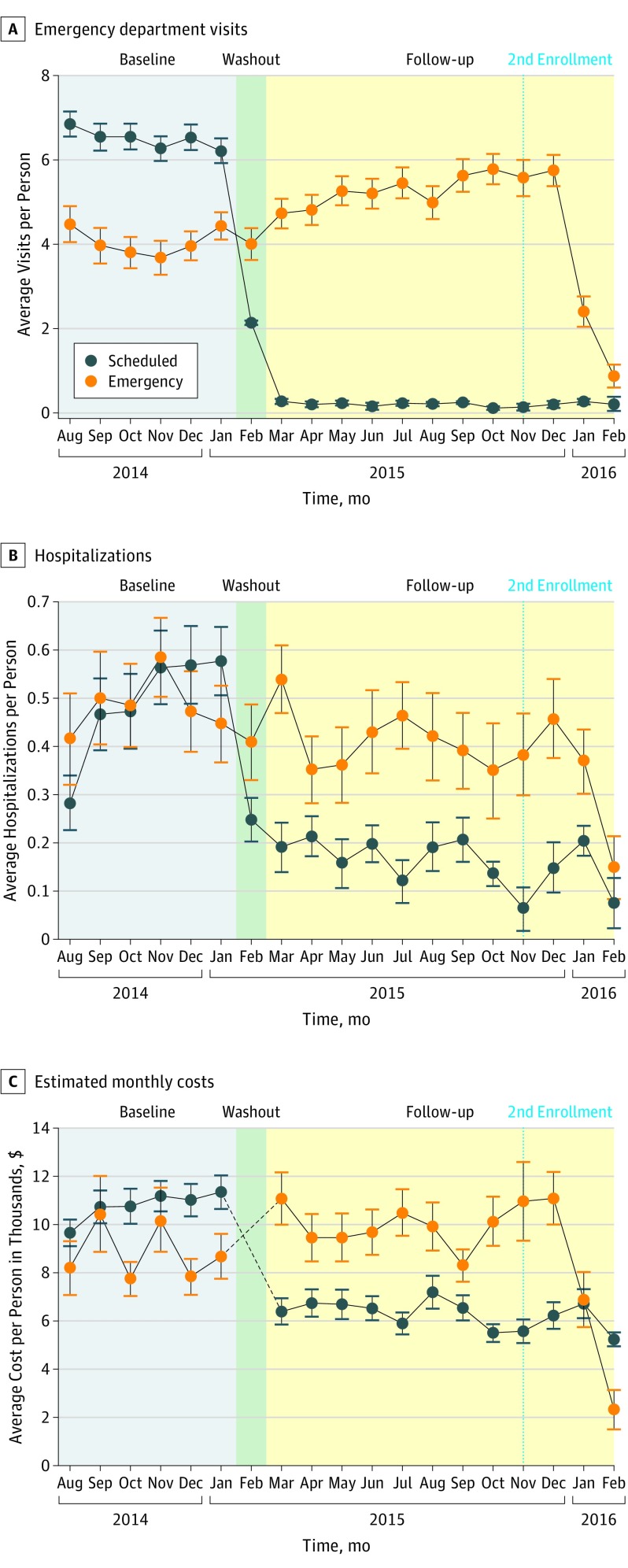
Design, setting, and participants: Observational cohort study of 181 eligible adults with ESRD receiving emergency-only dialysis in Dallas, Texas, who became newly eligible and applied for private commercial health insurance in February 2015; 105 received coverage and were enrolled in scheduled dialysis; 76 were not enrolled in insurance for nonclinical reasons (eg, lack of capacity at a participating outpatient dialysis center) and remained uninsured, receiving emergency-only dialysis. We examined data on eligible persons during a 6-month period prior to enrollment (baseline period, August 1, 2014-January 31, 2015) until 12 months after enrollment (follow-up period, March 1, 2015-February 29, 2016), with an intervening 1-month washout period (February 2015). All participants were undocumented immigrants; self-reported data on immigration status was collected from Parkland Hospital electronic health records.
Exposures: Enrollment in private health insurance coverage and scheduled dialysis.
Main outcomes and measures: We used enrollment in health insurance and scheduled dialysis to estimate the influence of scheduled dialysis on 1-year mortality, utilization, and health care costs, using a propensity score-adjusted, intention-to-treat approach, including time-to-event analyses for mortality, difference-in-differences (DiD) negative binomial regression analyses for utilization, and DiD gamma generalized linear regression for health care costs.
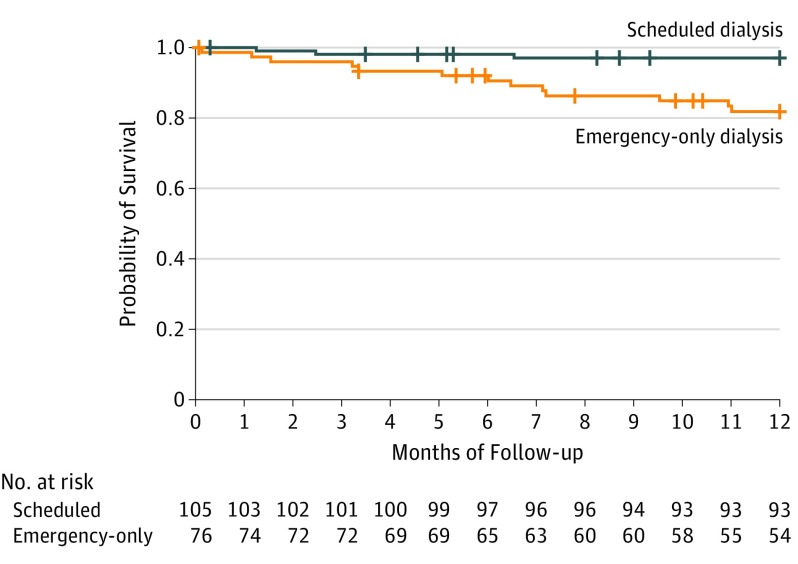
Results: Of 181 eligible adults with ESRD, 105 (65 men, 40 women; mean age, 45 years) received scheduled dialysis and 76 (38 men, 38 women; mean age, 52 years) received emergency-only dialysis. Compared with emergency-only dialysis, scheduled dialysis was significantly associated with reduced mortality (3% vs 17%, P = .001; absolute risk reduction, 14%; number needed to treat, 7; adjusted hazard ratio, 4.6; 95% CI, 1.2-18.2; P = .03), adjusted emergency department visits (-5.2 vs +1.1 visits/mo; DiD, -6.2; P < .001), adjusted hospitalizations (-2.1 vs -0.5 hospitalizations/6 months; DiD, -1.6; P < .001), adjusted hospital days (-9.2 vs +0.8 days/6 months; DiD, -9.9; P = .007), and adjusted costs (-$4316 vs +$1452 per person per month; DiD, -$5768; P < .001).
Conclusions and relevance: In this study, scheduled dialysis was significantly associated with reduced 1-year mortality, health care utilization, and costs compared with emergency-only dialysis. Scheduled dialysis should be the universal standard of care for all individuals with ESRD in the United States.
Conflict of interest statement
Figures
Comment in
-
Providing Comprehensive Health Care for Undocumented People in the United States.JAMA Intern Med. 2019 Feb 1;179(2):183-185. doi: 10.1001/jamainternmed.2018.5847. JAMA Intern Med. 2019. PMID: 30575858 No abstract available.
-
Evidence-based therapy for undocumented immigrants with ESRD.Nat Rev Nephrol. 2019 Jun;15(6):322-324. doi: 10.1038/s41581-019-0137-4. Nat Rev Nephrol. 2019. PMID: 30850751 No abstract available.
-
Comparison of Scheduled vs Emergency-Only Dialysis in Undocumented Immigrants With End-stage Renal Disease.JAMA Intern Med. 2019 May 1;179(5):728. doi: 10.1001/jamainternmed.2019.0540. JAMA Intern Med. 2019. PMID: 31058937 No abstract available.
-
Comparison of Scheduled vs Emergency-Only Dialysis in Undocumented Immigrants With End-stage Renal Disease-Reply.JAMA Intern Med. 2019 May 1;179(5):728-729. doi: 10.1001/jamainternmed.2019.0537. JAMA Intern Med. 2019. PMID: 31058944 No abstract available.
