

Clinical, Radiologic, and Prognostic Features of Myelitis Associated With Myelin Oligodendrocyte Glycoprotein Autoantibody
- PMID: 30575890
- PMCID: PMC6440233
- DOI: 10.1001/jamaneurol.2018.4053
Clinical, Radiologic, and Prognostic Features of Myelitis Associated With Myelin Oligodendrocyte Glycoprotein Autoantibody
Abstract
Importance: Recognizing the characteristics of myelin oligodendrocyte glycoprotein autoantibody (MOG-IgG) myelitis is essential for early accurate diagnosis and treatment.
Objective: To evaluate the clinical, radiologic, and prognostic features of MOG-IgG myelitis and compare with myelitis with aquaporin-4-IgG (AQP4-IgG) and multiple sclerosis (MS).
Design, setting, and participants: We retrospectively identified 199 MOG-IgG-positive Mayo Clinic patients from January 1, 2000, through December 31, 2017, through our neuroimmunology laboratory. Fifty-four patients met inclusion criteria of (1) clinical myelitis; (2) MOG-IgG positivity; and (3) medical records available. We excluded 145 patients without documented myelitis. Myelitis of AQP4-IgG (n = 46) and MS (n = 26) were used for comparison.
Main outcomes and measures: Outcome variables included modified Rankin score and need for gait aid. A neuroradiologist analyzed spine magnetic resonance imaging of patients with MOG-IgG and control patients blinded to diagnosis.
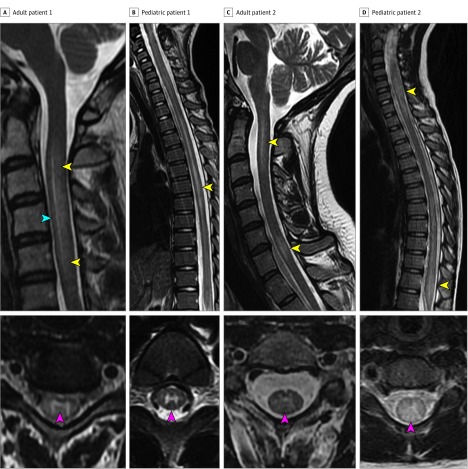
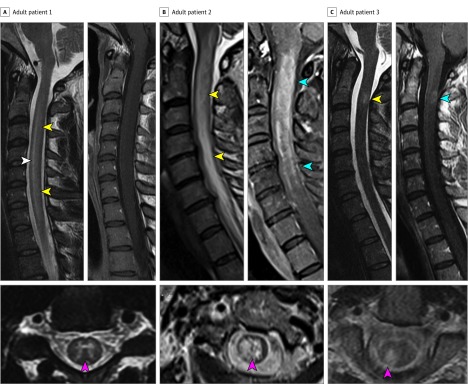
Results: Of 54 included patients with MOG-IgG myelitis, the median age was 25 years (range, 3-73 years) and 24 were women (44%). Isolated transverse myelitis was the initial manifestation in 29 patients (54%), and 10 (19%) were initially diagnosed as having viral/postviral acute flaccid myelitis. Cerebrospinal fluid-elevated oligoclonal bands occurred in 1 of 38 (3%). At final follow-up (median, 24 months; range, 2-120 months), 32 patients (59%) had developed 1 or more relapses of optic neuritis (n = 31); transverse myelitis (n = 7); or acute disseminated encephalomyelitis (n = 1). Clinical features favoring MOG-IgG myelitis vs AQP4-IgG or MS myelitis included prodromal symptoms and concurrent acute disseminated encephalomyelitis. Magnetic resonance imaging features favoring MOG-IgG over AQP4-IgG or MS myelitis were T2-signal abnormality confined to gray matter (sagittal line and axial H sign) and lack of enhancement. Longitudinally extensive T2 lesions were of similar frequency in MOG-IgG and AQP4-IgG myelitis (37 of 47 [79%] vs 28 of 34 [82%]; P = .52) but not found in MS. Multiple spinal cord lesions and conus involvement were more frequent with MOG-IgG than AQP4-IgG but not different from MS. Wheelchair dependence at myelitis nadir occurred in one-third of patients with MOG-IgG and AQP4-IgG but never with MS, although patients with MOG-IgG myelitis recovered better than those with AQP4-IgG.
Conclusions and relevance: Myelitis is an early manifestation of MOG-IgG-related disease and may have a clinical phenotype of acute flaccid myelitis. We identified a variety of clinical and magnetic resonance imaging features that may help clinicians identify those at risk in whom MOG-IgG should be tested.
Conflict of interest statement
Figures
References
-
- Greenberg BM. Treatment of acute transverse myelitis and its early complications. Continuum (Minneap Minn). 2011;17(4):733-743. - PubMed
-
- Zalewski NL, Flanagan EP, Keegan BM. Evaluation of idiopathic transverse myelitis revealing specific myelopathy diagnoses. Neurology. 2018;90(2):e96-e102. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
