

Role of Screening History in Clinical Meaning and Optimal Management of Positive Cervical Screening Results
- PMID: 30576462
- PMCID: PMC6695308
- DOI: 10.1093/jnci/djy192
Role of Screening History in Clinical Meaning and Optimal Management of Positive Cervical Screening Results
Abstract
Background: Cervical cancer is caused by persistent human papillomavirus (HPV) infection. US consensus management guidelines for a positive cervical screening result typically focus on the current screening result only. A negative testing history may alter risk of the following positive screening results, caused by a new HPV infection, and therefore its optimal management.
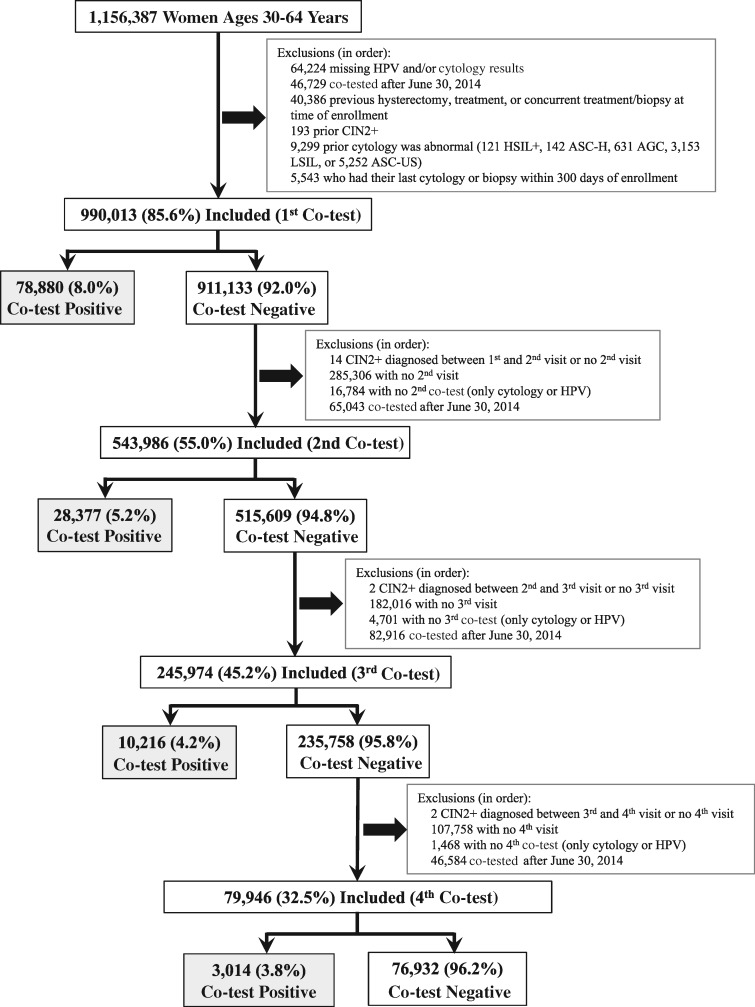
Methods: Women ages 30 years and older were screened with triennial HPV and cytology co-testing at Kaiser Permanente Northern California from 2003 to 2014. We estimated the subsequent 5-year risks of cervical intraepithelial neoplasia grade 3 or more severe diagnoses (CIN3+) in a cohort of 1 156 387 women following abnormal (atypical squamous cells of undetermined significance [ASC-US] or worse) cytology and/or positive HPV testing, when the test result followed 0 (n = 990 013), 1 (n = 543 986), 2 (n = 245 974), or 3 (n = 79 946) consecutive negative co-test(s). All statistical tests were two-sided.
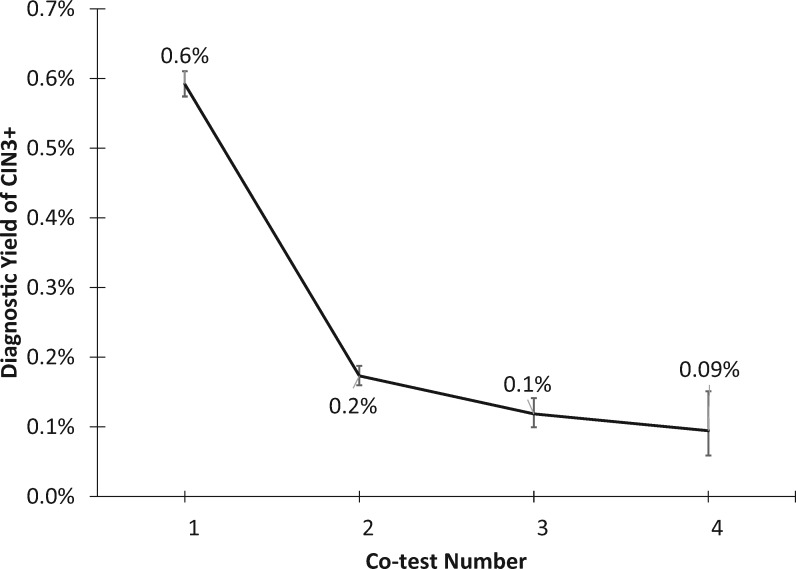
Results: Following 0-3 successive negative co-tests, 5-year CIN3+ risks following a positive HPV test decreased progressively from 7.2% (95% CI = 7.0% to 7.4%) to 1.5% (95% CI = 0.7% to 3.4%) (Ptrend < .001). Similarly, risks following an abnormal (ASC-US or worse) cytology result decreased from 6.6% (95% CI = 6.4% to 6.9%) to 1.1% (95% CI = 0.5% to 2.3%) (Ptrend < .001). Risks following low-grade squamous intraepithelial lesion, the risk threshold for referral to colposcopy in the United States, decreased from 5.2% (95% CI = 4.7% to 5.7%) to 0.9% (95% CI = 0.2% to 4.3%). Risks following high-grade squamous intraepithelial lesion or more severe, a specific marker for the presence of precancerous lesions, decreased from 50.0% (95% CI = 47.5% to 52.5%) to 10.0% (95% CI = 2.6% to 34.4%).
Conclusions: Following one or more sequential antecedent, documented negative co-tests or HPV tests, women with HPV-positive ASC-US or low-grade squamous intraepithelial lesion might have sufficiently low CIN3+ risk that they do not need colposcopy referral and might instead undergo 6-12-month surveillance for evidence of higher risk before being referred to colposcopy.
© The Author(s) 2018. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Performance of carcinogenic human papillomavirus (HPV) testing and HPV16 or HPV18 genotyping for cervical cancer screening of women aged 25 years and older: a subanalysis of the ATHENA study.Lancet Oncol. 2011 Sep;12(9):880-90. doi: 10.1016/S1470-2045(11)70188-7. Epub 2011 Aug 22. Lancet Oncol. 2011. PMID: 21865084 Clinical Trial.
-
Follow-up testing after colposcopy: five-year risk of CIN 2+ after a colposcopic diagnosis of CIN 1 or less.J Low Genit Tract Dis. 2013 Apr;17(5 Suppl 1):S69-77. doi: 10.1097/LGT.0b013e31828543b1. J Low Genit Tract Dis. 2013. PMID: 23519308 Free PMC article.
-
The clinician's view: role of human papillomavirus testing in the American Society for Colposcopy and Cervical Pathology Guidelines for the management of abnormal cervical cytology and cervical cancer precursors.Arch Pathol Lab Med. 2003 Aug;127(8):950-8. doi: 10.5858/2003-127-950-TCVROH. Arch Pathol Lab Med. 2003. PMID: 12952506
-
Cervical Cancer Screening: A Review.JAMA. 2023 Aug 8;330(6):547-558. doi: 10.1001/jama.2023.13174. JAMA. 2023. PMID: 37552298 Review.
-
Human papillomavirus testing in primary cervical screening and abnormal Papanicolaou management.Obstet Gynecol Surv. 2006 Jun;61(6 Suppl 1):S15-25. doi: 10.1097/01.ogx.0000221011.01750.25. Obstet Gynecol Surv. 2006. PMID: 16729900 Review.
Cited by
-
Overexpression of long non-coding RNA WT1-AS or silencing of PIK3AP1 are inhibitory to cervical cancer progression.Cell Cycle. 2021 Dec;20(24):2583-2596. doi: 10.1080/15384101.2021.1991106. Epub 2021 Nov 28. Cell Cycle. 2021. PMID: 34839795 Free PMC article.
-
The Improving Risk Informed HPV Screening (IRIS) Study: Design and Baseline Characteristics.Cancer Epidemiol Biomarkers Prev. 2022 Feb;31(2):486-492. doi: 10.1158/1055-9965.EPI-21-0865. Epub 2021 Nov 17. Cancer Epidemiol Biomarkers Prev. 2022. PMID: 34789470 Free PMC article.
-
Human Papillomavirus Intermittence and Risk Factors Associated With First Detections and Redetections in the Ludwig-McGill Cohort Study of Adult Women.J Infect Dis. 2023 Aug 16;228(4):402-411. doi: 10.1093/infdis/jiad043. J Infect Dis. 2023. PMID: 36790831 Free PMC article.
-
2019 ASCCP Risk-Based Management Consensus Guidelines: Methods for Risk Estimation, Recommended Management, and Validation.J Low Genit Tract Dis. 2020 Apr;24(2):90-101. doi: 10.1097/LGT.0000000000000528. J Low Genit Tract Dis. 2020. PMID: 32243306 Free PMC article.
-
Women with a positive high-risk human papillomavirus (HPV) test remain at increased risk of HPV infection and cervical precancer ≥15 years later.Tumour Virus Res. 2022 Dec;14:200240. doi: 10.1016/j.tvr.2022.200240. Epub 2022 May 28. Tumour Virus Res. 2022. PMID: 35640823 Free PMC article.
References
-
- Walboomers JMM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;1891:12–19. - PubMed
-
- Castle PE, Kinney WK, Xue X, et al. Effect of several negative rounds of human papillomavirus and cytology co-testing on safety against cervical cancer. Ann Intern Med. 2018;1681:20–29. - PubMed
