

Advance Directives, Medical Conditions, and Preferences for End-of-Life Care Among Physicians: 12-year Follow-Up of the Johns Hopkins Precursors Study
- PMID: 30576712
- PMCID: PMC6382559
- DOI: 10.1016/j.jpainsymman.2018.12.328
Advance Directives, Medical Conditions, and Preferences for End-of-Life Care Among Physicians: 12-year Follow-Up of the Johns Hopkins Precursors Study
Abstract
Context: Stability of preferences for life-sustaining treatment may vary depending on personal characteristics.
Objective: We estimated the stability of preferences for end-of-life treatment over 12 years and whether advance directives and medical conditions were associated with change in preferences for end-of-life treatment.
Design: Mailed survey of older physicians.
Methods: Longitudinal cohort study of medical students in the graduating classes from 1948 to 1964 at Johns Hopkins University. Eight hundred ninety eight physicians who completed the life-sustaining treatment questionnaire anytime in 1999, 2002, 2005, and 2011 (mean age 68.2 years at baseline). Preferences for life-sustaining treatment were assessed using a checklist questionnaire in response to a standard "brain injury" scenario and considered as a package using the latent class transition model.
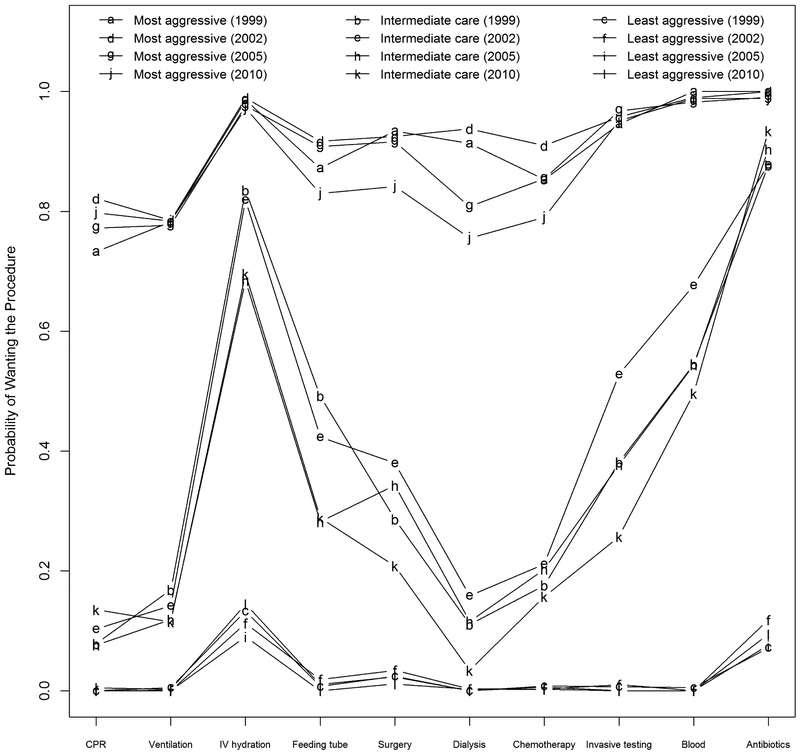
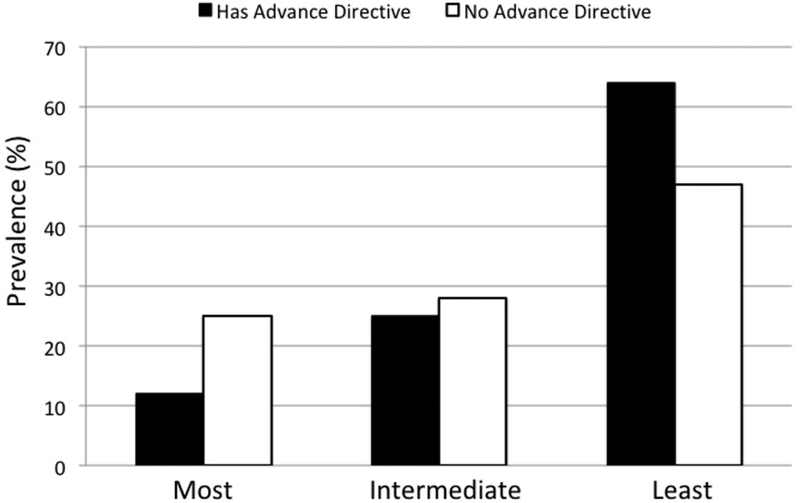
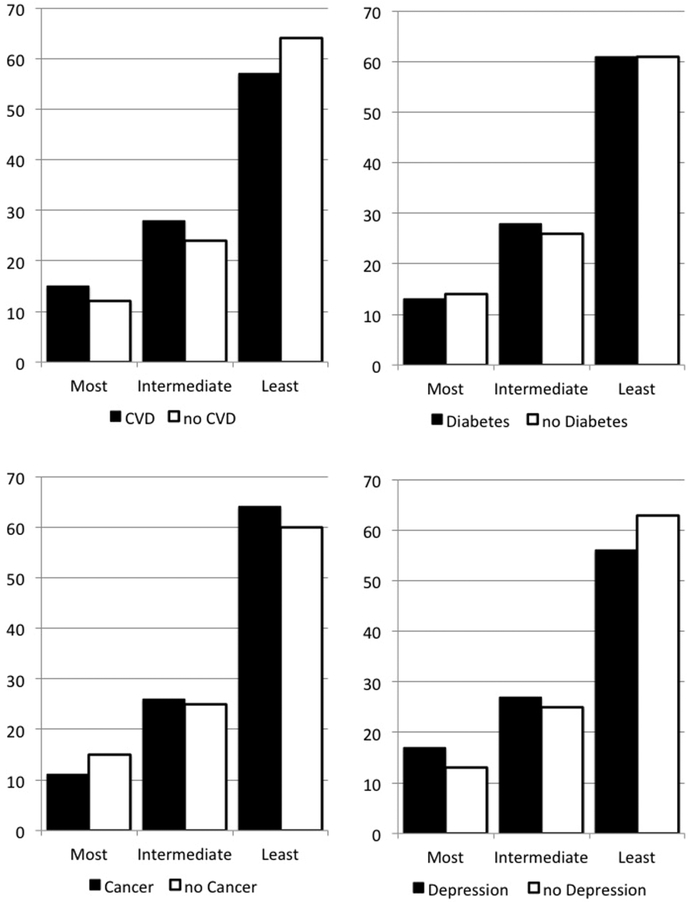
Results: End-of-life preferences grouped into three classes: most aggressive (wanting most interventions; 14% of physicians), least aggressive (declining most interventions; 61%), and an intermediate class (declining most interventions except intravenous fluids and antibiotics; 25%). Physicians without an advance directive were more likely to desire more treatment and were less likely to transition out the most aggressive class. Transition probabilities from class to class did not vary over time. Persons with cancer expressed preference for the least aggressive treatment, whereas persons with cardiovascular disease and depression had preferences for more aggressive treatment.
Conclusion: Transitions in end-of-life preferences and the factors influencing change and stability suggest that periodic reassessment for planning end-of-life care is needed.
Keywords: End-of-life preferences; advance directives; latent transition analysis.
Copyright © 2018 American Academy of Hospice and Palliative Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure and Acknowledgements:
The authors declare no conflicts of interest.
Figures
Similar articles
-
Stability of preferences for end-of-life treatment after 3 years of follow-up: the Johns Hopkins Precursors Study.Arch Intern Med. 2008 Oct 27;168(19):2125-30. doi: 10.1001/archinte.168.19.2125. Arch Intern Med. 2008. PMID: 18955642 Free PMC article.
-
Life-sustaining treatments: what do physicians want and do they express their wishes to others?J Am Geriatr Soc. 2003 Jul;51(7):961-9. doi: 10.1046/j.1365-2389.2003.51309.x. J Am Geriatr Soc. 2003. PMID: 12834516
-
Physical functioning, depression, and preferences for treatment at the end of life: the Johns Hopkins Precursors Study.J Am Geriatr Soc. 2004 Apr;52(4):577-82. doi: 10.1111/j.1532-5415.2004.52165.x. J Am Geriatr Soc. 2004. PMID: 15066074
-
The need for safeguards in advance care planning.J Gen Intern Med. 2012 May;27(5):595-600. doi: 10.1007/s11606-011-1976-2. Epub 2012 Jan 12. J Gen Intern Med. 2012. PMID: 22237664 Free PMC article. Review.
-
End-of-life communication in Korean older adults: With focus on advance care planning and advance directives.Geriatr Gerontol Int. 2016 Apr;16(4):407-15. doi: 10.1111/ggi.12603. Epub 2015 Oct 13. Geriatr Gerontol Int. 2016. PMID: 26459613 Review.
Cited by
-
Preference for Aggressive End-of-Life Care among Advanced Cancer Patients in Wuhan, China: A Cross-Sectional Study.Int J Environ Res Public Health. 2020 Sep 10;17(18):6592. doi: 10.3390/ijerph17186592. Int J Environ Res Public Health. 2020. PMID: 32927824 Free PMC article.
-
Psychosocial Factors Associated With Thoughts Regarding Life-Sustaining Treatment for Oneself and Family Members.Psychiatry Investig. 2024 Jun;21(6):646-654. doi: 10.30773/pi.2024.0032. Epub 2024 Jun 24. Psychiatry Investig. 2024. PMID: 38960442 Free PMC article.
-
Associations between physicians' personal preferences for end-of-life decisions and their own clinical practice: PROPEL survey study in Europe, North America, and Australia.Palliat Med. 2025 Feb;39(2):266-276. doi: 10.1177/02692163241300853. Epub 2024 Dec 13. Palliat Med. 2025. PMID: 39668726 Free PMC article.
-
Indian Society of Critical Care Medicine and Indian Association of Palliative Care Expert Consensus and Position Statements for End-of-life and Palliative Care in the Intensive Care Unit.Indian J Crit Care Med. 2024 Mar;28(3):200-250. doi: 10.5005/jp-journals-10071-24661. Indian J Crit Care Med. 2024. PMID: 38477011 Free PMC article.
-
Mixed methods grant applications in the health sciences: An analysis of reviewer comments.PLoS One. 2019 Nov 15;14(11):e0225308. doi: 10.1371/journal.pone.0225308. eCollection 2019. PLoS One. 2019. PMID: 31730660 Free PMC article.
References
-
- Epstein RM, Duberstein PR, Fenton JJ, Fiscella K, Hoerger M, Tancredi DJ, et al. Effect of a Patient-Centered Communication Intervention on Oncologist-Patient Communication, Quality of Life, and Health Care Utilization in Advanced Cancer: The VOICE Randomized Clinical Trial. JAMA Oncol. 2017;3(1):92–100. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
