

Effect of all-extremity high-intensity interval training vs. moderate-intensity continuous training on aerobic fitness in middle-aged and older adults with type 2 diabetes: A randomized controlled trial
- PMID: 30576716
- PMCID: PMC6404965
- DOI: 10.1016/j.exger.2018.12.013
Effect of all-extremity high-intensity interval training vs. moderate-intensity continuous training on aerobic fitness in middle-aged and older adults with type 2 diabetes: A randomized controlled trial
Abstract
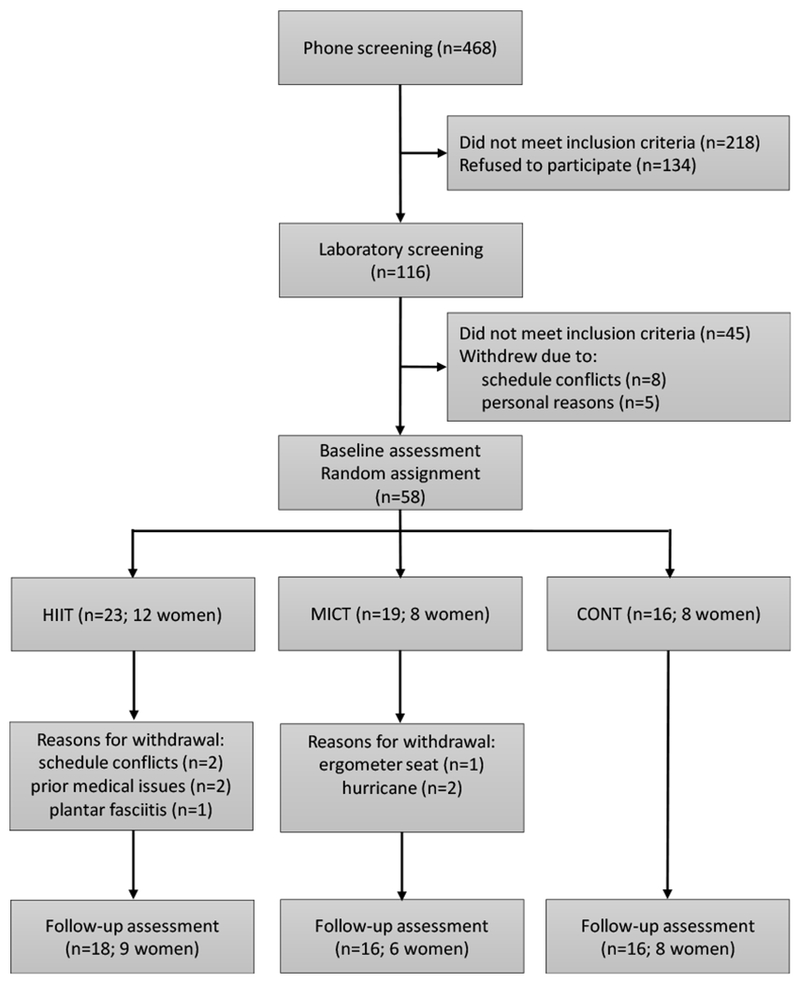
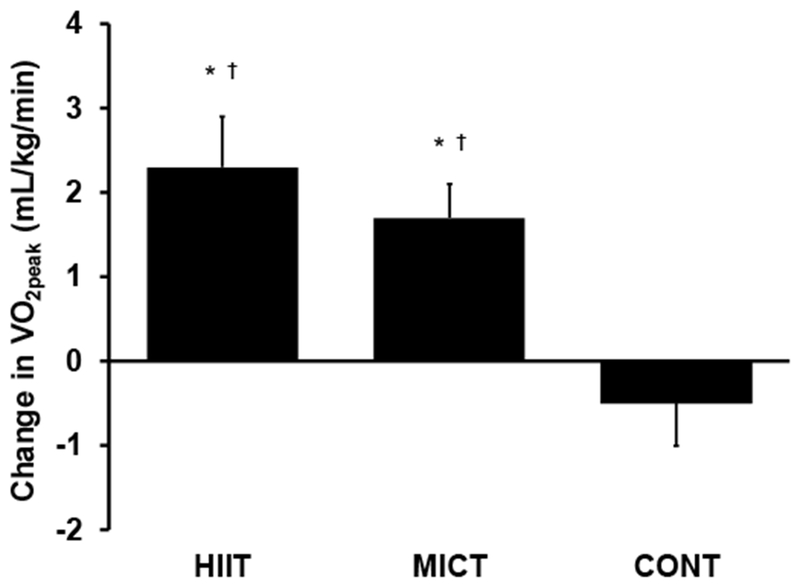
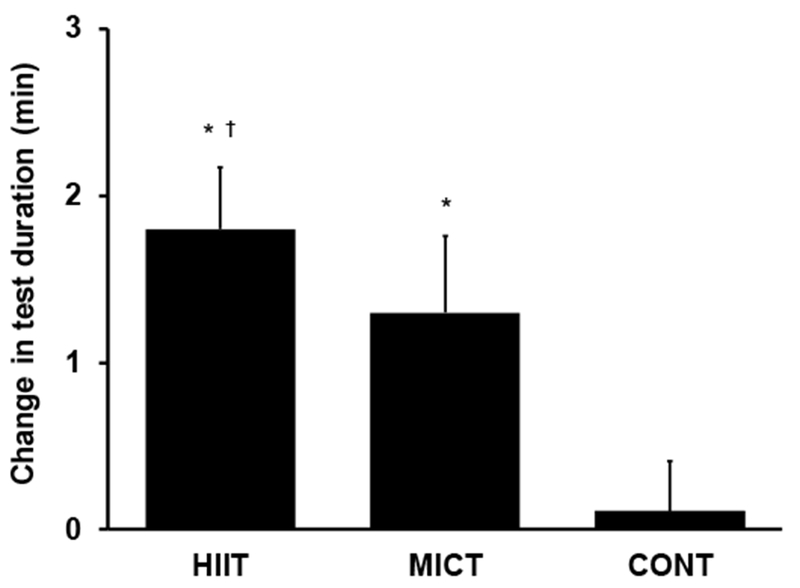
Aging and diabetes are associated with decreased aerobic fitness, an independent predictor of mortality. Aerobic exercise is prescribed to improve aerobic fitness; however, middle-aged/older diabetic patients often suffer from mobility limitations which restrict walking. Non-weight-bearing/low-impact exercise is recommended but the optimal exercise prescription is uncertain. The goal of this randomized controlled trial was twofold: 1) to test if high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT), implemented on a non-weight-bearing all-extremity ergometer, are feasible, well-tolerated and safe in middle-aged/older adults with type 2 diabetes; and 2) to test whether all-extremity HIIT is more effective in improving aerobic fitness than MICT. A total of 58 sedentary individuals with type 2 diabetes (46 to 78 years; 63 ± 1) were randomized to all-extremity HIIT (n = 23), MICT (n = 19) or non-exercise control (CONT; n = 16). All-extremity HIIT and MICT, performed 4×/week for 8 weeks under supervision, resulted in no adverse events requiring hospitalization or medical treatment. Aerobic fitness (VO2peak) improved by 10% in HIIT and 8% in MICT and maximal exercise tolerance increased by 1.8 and 1.3 min, respectively (P ≤ 0.002 vs. baseline; P ≥ 0.9 for HIIT vs. MICT). In conclusion, all-extremity HIIT and MICT are feasible, well-tolerated and safe and result in similar improvements in aerobic fitness in middle-aged/older individuals with type 2 diabetes. These findings have important implications for exercise prescription for diabetic patients; they indicate that all-extremity exercise is a feasible alternative to weight-bearing exercise and those who are unable or unwilling to engage in HIIT may receive similar benefits from MICT.
Keywords: Aerobic fitness; Aging; All-extremity aerobic exercise; Cardiovascular disease risk; Diabetes; VO(2peak).
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Albright AL, 2013. Diabetes, in: Ehrman JK, Gordon PM, Visich PS, Keteyian SJ (Eds.), Clinical Exercise Physiology, Human Kinetics, Champaign, 91–112.
-
- Amundsen BH, Rognmo O, Hatlen-Rebhan G, Slordahl SA, 2008. High-intensity aerobic exercise improves diastolic function in coronary artery disease, Scand Cardiovasc J. 42, 110–117. - PubMed
-
- Awotidebe TO, Adedoyin RA, Oke KI, Ativie RN, Opiyo R, Ikujeyisi EO, Ikem RT, Afolabi MA, 2017. Relationship between functional capacity and health-related quality of life of patients with type-2 diabetes, Diabetes Metab Syndr. 11, 1–5. - PubMed
-
- Beaver WL, Wasserman K, Whipp BJ, 1986. A new method for detecting anaerobic threshold by gas exchange, J Appl Physiol (1985). 60, 2020–2027. - PubMed
-
- Boule NG, Haddad E, Kenny GP, Wells GA, Sigal RJ, 2001. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials, JAMA. 286, 1218–1227. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
