

A WHO-HPH operational program versus usual routines for implementing clinical health promotion: an RCT in health promoting hospitals (HPH)
- PMID: 30577871
- PMCID: PMC6304000
- DOI: 10.1186/s13012-018-0848-0
A WHO-HPH operational program versus usual routines for implementing clinical health promotion: an RCT in health promoting hospitals (HPH)
Abstract
Background: Implementation of clinical health promotion (CHP) aiming at better health gain is slow despite its effect. CHP focuses on potentially modifiable lifestyle risks such as smoking, alcohol, diet, and physical inactivity. An operational program was created to improve implementation. It included patients, staff, and the organization, and it combined existing standards, indicators, documentation models, a performance recognition process, and a fast-track implementation model. The aim of this study was to evaluate if the operational program improved implementation of CHP in clinical hospital departments, as measured by health status of patients and staff, frequency of CHP service delivery, and standards compliance.
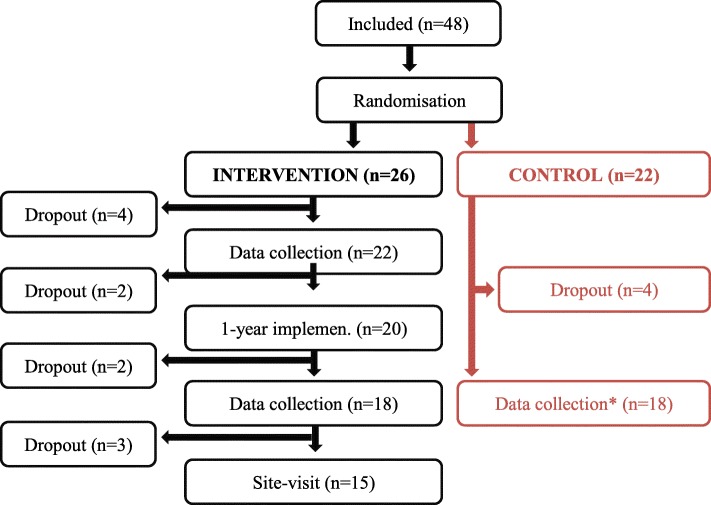
Methods: Forty-eight hospital departments were recruited via open call and stratified by country. Departments were assigned to the operational program (intervention) or usual routine (control group). Data for analyses included 36 of these departments and their 5285 patients (median 147 per department; range 29-201), 2529 staff members (70; 10-393), 1750 medical records (50; 50-50), and standards compliance assessments. Follow-up was measured after 1 year. The outcomes were health status, service delivery, and standards compliance.
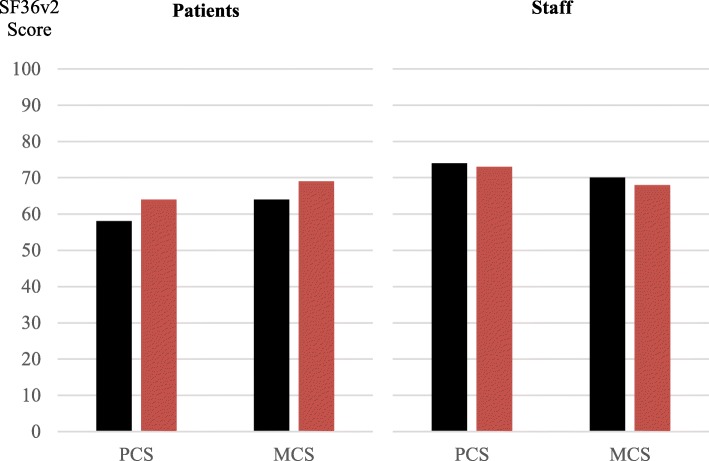
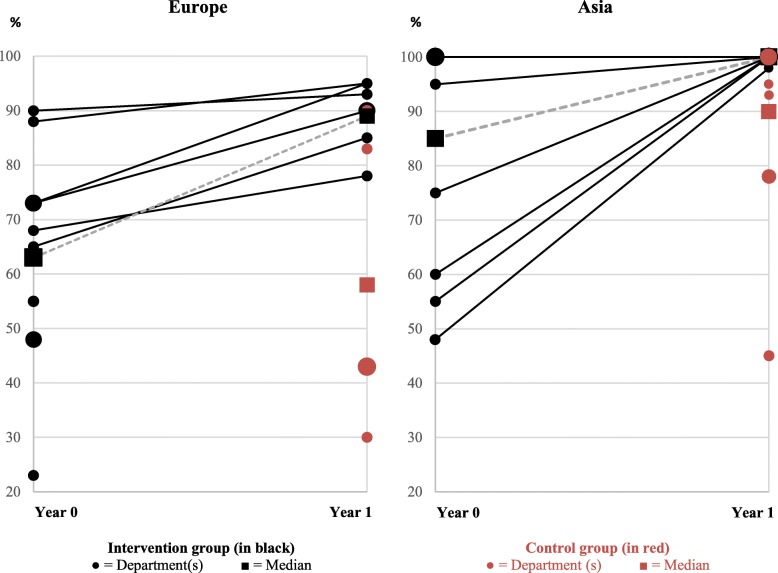
Results: No health differences between groups were found, but the intervention group had higher identification of lifestyle risk (81% versus 60%, p < 0.01), related information/short intervention and intensive intervention (54% versus 39%, p < 0.01 and 43% versus 25%, p < 0.01, respectively), and standards compliance (95% versus 80%, p = 0.02).
Conclusions: The operational program improved implementation by way of lifestyle risk identification, CHP service delivery, and standards compliance. The unknown health effects, the bias, and the limitations should be considered in implementation efforts and further studies.
Trial registration: ClinicalTrials.gov : NCT01563575. Registered 27 March 2012. https://clinicaltrials.gov/ct2/show/NCT01563575.
Keywords: Clinical health promotion; Fast-track implementation; Health promoting hospitals; Hospital staff; Lifestyle risk; Patients; Quality improvement; Strategic implementation.
Conflict of interest statement
Ethics approval and consent to participate
All data were anonymized at the source, and no person-identifiable information was recorded or transferred. The study included no biological material. The anonymized data were stored and secured by Capital Region Denmark CIMT. Paper records were maintained under double lock. Only the international research team had access to all data. The study was approved by the Internal Review Board of Bispebjerg-Frederiksberg Hospital, University of Copenhagen, Denmark, and by the Danish Data Protection Agency (j.nr. 2012-41-0152 / 2017-41-5029). All participating departments had local approval from their internal review body, department head, and hospital management. Participation in the study was not associated with any risks. The time required to complete forms and surveys was considered a minor inconvenience.
Consent for publication
All participating clinical departments that delivered data obtained local approval from their internal review body, approval from the head of the department, and from the hospital management. Consent from individual patients or staff was not required as no person-identifiable data was captured at any point.
Competing interests
All authors completed the ICMJE uniform disclosure form at
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Balas EA, Boren SA. Yearbook of medical informatics: managing clinical knowledge for health care improvement. Stuttgart: Schattauer Verlagsgesellschaft mbH; 2000. - PubMed
-
- World health organization. Ottawa charter for health promotion. Health Promot Int. 1986;1(4):405.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
