

Characterization of diabetes following pancreatic surgery in patients with congenital hyperinsulinism
- PMID: 30577875
- PMCID: PMC6304089
- DOI: 10.1186/s13023-018-0970-8
Characterization of diabetes following pancreatic surgery in patients with congenital hyperinsulinism
Abstract
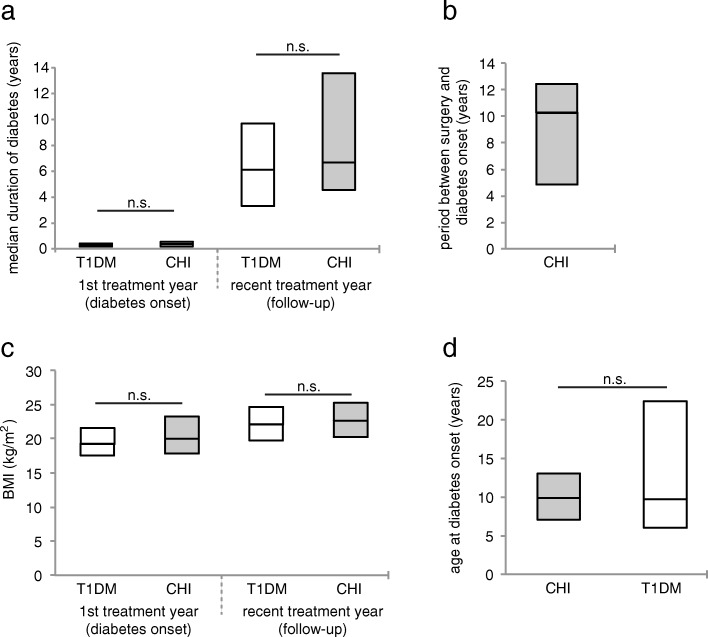
Background: Congenital hyperinsulinism (CHI) is the most common cause of persistent hypoglycaemia in infancy that leads to unfavourable neurological outcome if not treated adequately. In patients with severe diffuse CHI it remains under discussion whether pancreatic surgery should be performed or intensive medical treatment with the acceptance of recurrent episodes of mild hypoglycaemia is justified. Near-total pancreatectomy is associated with high rates of insulin-dependent diabetes mellitus and exocrine pancreatic insufficiency. Little is known about the management and long-term glycaemic control of CHI patients with diabetes after pancreatic surgery. We searched the German/Austrian DPV database and compared the course of 42 CHI patients with diabetes to that of patients with type 1 diabetes mellitus (T1DM). Study groups were compared at diabetes onset and after a follow-up period of 6.1 [3.3-9.7] (median [interquartile range]) years.
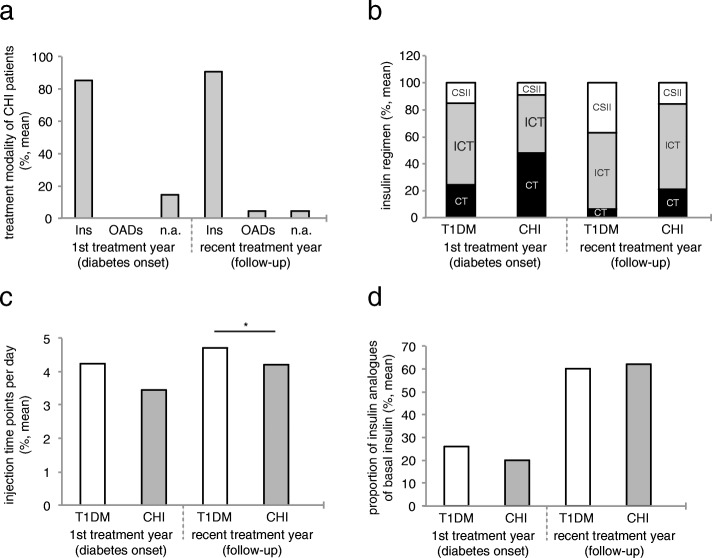
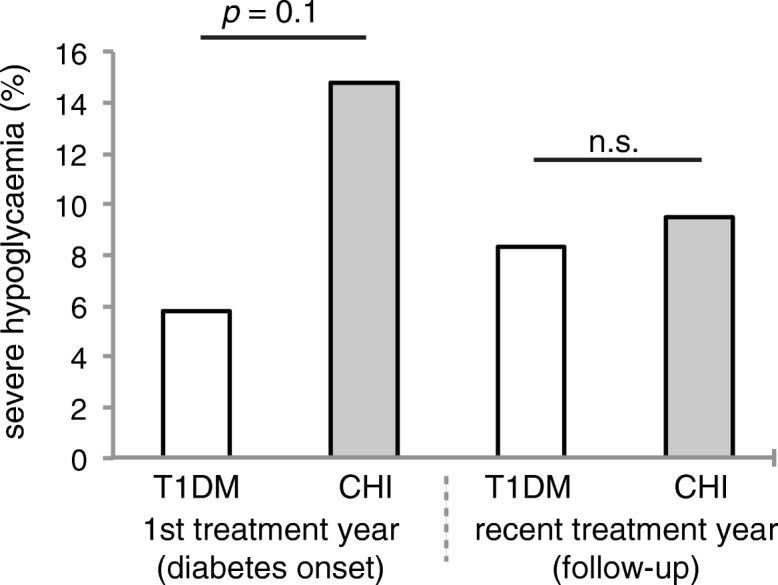
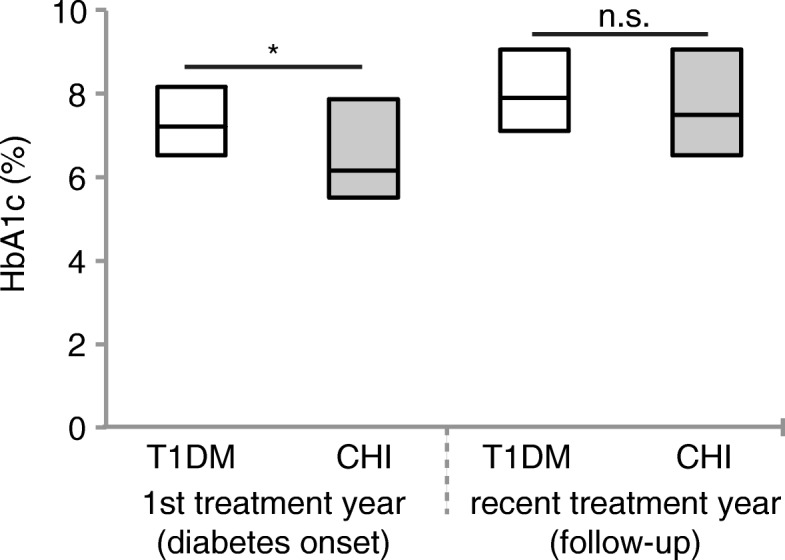
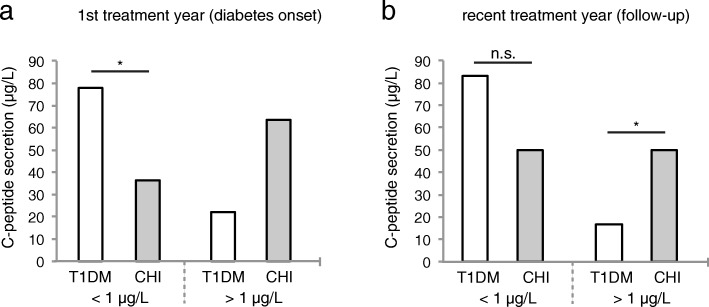
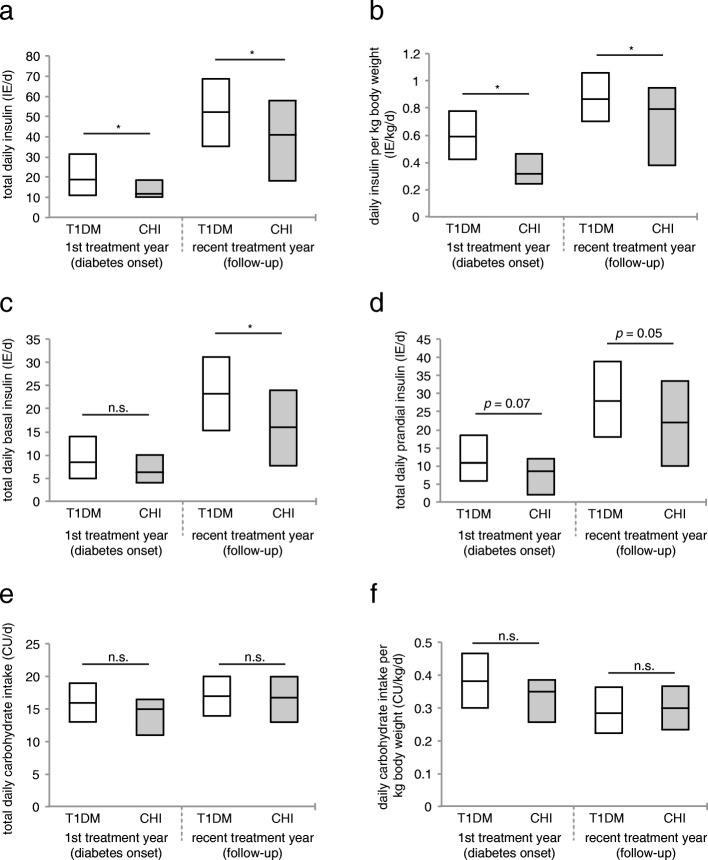
Results: The majority of CHI patients with diabetes were treated with insulin (85.2% [70.9-99.5] at diabetes onset, and 90.5% [81.2-99.7] at follow-up). However, compared to patients with T1DM, significantly more patients in the CHI group with diabetes were treated with conventional insulin therapy (47.8% vs. 24.4%, p = 0.03 at diabetes onset, and 21.1% vs. 6.4% at follow-up, p = 0.003), and only a small number of CHI patients were treated with insulin pumps. Daily insulin dose was significantly lower in CHI patients with diabetes than in patients with T1DM, both at diabetes onset (0.3 [0.2-0.5] vs. 0.6 IE/kg/d [0.4-0.8], p = 0.003) and follow-up (0.8 [0.4-1.0] vs. 0.9 [0.7-1.0] IE/kg/d, p = 0.02), while daily carbohydrate intake was comparable in both groups. Within the first treatment year, HbA1c levels were significantly lower in CHI patients with diabetes (6.2% [5.5-7.9] vs. 7.2% [6.5-8.2], p = 0.003), but increased to a level comparable to that of T1DM patients at follow-up. Interestingly, in CHI patients, the risk of severe hypoglycaemia tends to be higher only at diabetes onset (14.8% vs. 5.8%, p = 0.1).
Conclusions: In surgically treated CHI patients insulin treatment needs to be intensified in order to achieve good glycaemic control. Our data furthermore emphasize the need for improved medical treatment options for patients with diazoxide- and/or octreotide-unresponsive CHI.
Keywords: Congenital hyperinsulinism; DPV initiative; Diabetes; Pancreatectomy.
Conflict of interest statement
Ethics approval and consent to participate
The DPV initiative and the analysis of anonymized data related to quality of care were approved by the ethics committee of the University of Ulm. The institutional review boards at each participating centre confirmed protection of patient primary rights.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- De Leon DD, Stanley CA. Congenital hypoglycemia disorders: new aspects of etiology, diagnosis, treatment and outcomes: highlights of the proceedings of the congenital hypoglycemia disorders symposium, Philadelphia April 2016. Pediatr Diabetes. 2017;18(1):3–9. doi: 10.1111/pedi.12453. - DOI - PMC - PubMed
-
- Helleskov A, Melikyan M, Globa E, Shcherderkina I, Poertner F, Larsen AM, Filipsen K, Brusgaard K, Christiansen CD, Hansen LK, et al. Both Low Blood Glucose and Insufficient Treatment Confer Risk of Neurodevelopmental Impairment in Congenital Hyperinsulinism: A Multinational Cohort Study. Front Endocrinol (Lausanne) 2017;8:156. doi: 10.3389/fendo.2017.00156. - DOI - PMC - PubMed
-
- Levy-Shraga Y, Pinhas-Hamiel O, Kraus-Houminer E, Landau H, Mazor-Aronovitch K, Modan-Moses D, Gillis D, Koren I, Dollberg D, Gabis LV. Cognitive and developmental outcome of conservatively treated children with congenital hyperinsulinism. J Pediatr Endocrinol Metab. 2013;26(3–4):301–308. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
