

Presentation, diagnosis and clinical course of the spectrum of progressive-fibrosing interstitial lung diseases
- PMID: 30578335
- PMCID: PMC9489068
- DOI: 10.1183/16000617.0076-2018
Presentation, diagnosis and clinical course of the spectrum of progressive-fibrosing interstitial lung diseases
Abstract
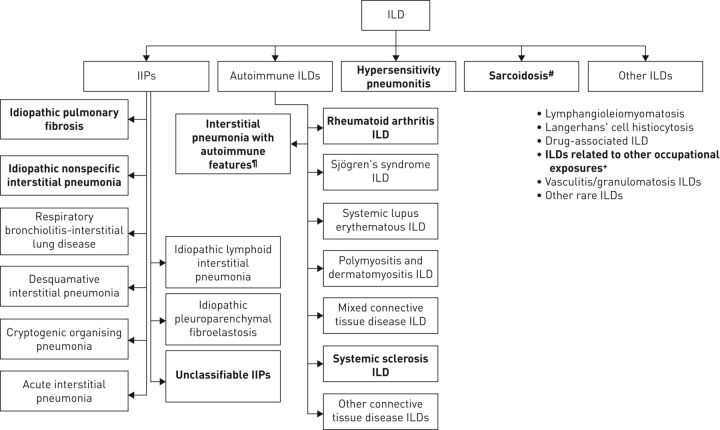
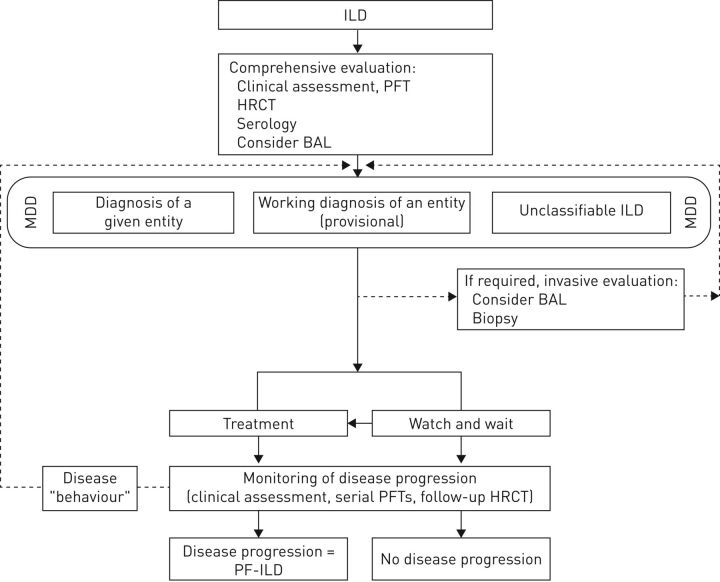
Although these conditions are rare, a proportion of patients with interstitial lung diseases (ILDs) may develop a progressive-fibrosing phenotype. Progressive fibrosis is associated with worsening respiratory symptoms, lung function decline, limited response to immunomodulatory therapies, decreased quality of life and, potentially, early death. Idiopathic pulmonary fibrosis may be regarded as a model for other progressive-fibrosing ILDs. Here we focus on other ILDs that may present a progressive-fibrosing phenotype, namely idiopathic nonspecific interstitial pneumonia, unclassifiable idiopathic interstitial pneumonia, connective tissue disease-associated ILDs (e.g. rheumatoid arthritis-related ILD), fibrotic chronic hypersensitivity pneumonitis, fibrotic chronic sarcoidosis and ILDs related to other occupational exposures. Differential diagnosis of these ILDs can be challenging, and requires detailed consideration of clinical, radiological and histopathological features. Accurate and early diagnosis is crucial to ensure that patients are treated optimally.
Copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: V. Cottin reports receiving the following, outside the submitted work: personal fees from Actelion for consultancy, lectures and travel to medical meetings; personal fees from Boehringer Ingelheim for the development of educational presentations, consultancy, lectures and travel to medical meetings; personal fees from Bayer for consultancy; personal fees from Gilead for acting as a member of an adjudication committee; personal fees from GSK for consultancy; personal fees from MSD for consultancy and travel to medical meetings; personal fees from Novartis for consultancy and lectures; personal fees from Roche for consultancy, lecture fees and travel to medical meetings; personal fees from Sanofi for consultancy and lectures; a grant to his institution from Boehringer Ingelheim; a grant to his institution from Roche; personal fees from Promedior for acting as Chair of the DSMB; personal fees from Celgene for the DSMB; and personal fees from Galapagos for consultancy and for acting as Chair of the DSMB. Conflict of interest: N.A. Hirani has nothing to disclose. Conflict of interest: D.L. Hotchkin has nothing to disclose. Conflict of interest: A.M. Nambiar reports receiving the following, outside the submitted work: grants, personal fees, non-financial support and other support from Boehringer Ingelheim; and grants from Genentech-Roche. Conflict of interest: T. Ogura reports receiving the following, outside the submitted work: grants and personal fees from Boehringer Ingelheim, Japan; grants from the Ministry of Health, Labour and Welfare, Japan; personal fees from Astellas Pharma Inc., Shionogi & Co. Ltd, Toray Industries Inc., AstraZeneca K.K. and Kyorin Inc. Conflict of interest: M. Otaola has nothing to disclose. Conflict of interest: D. Skowasch reports receiving the following, outside the submitted work: personal fees/honoraria for consulting and speaking from Boehringer Ingelheim and Roche. Conflict of interest: J.S. Park has nothing to disclose. Conflict of interest: H.K. Poonyagariyagorn has nothing to disclose. Conflict of interest: W. Wuyts reports receiving the following, outside the submitted work: grants paid to his university from Boehringer Ingelheim and Hoffmann La Roche; and travel fees from Galapagos. Conflict of interest: A.U. Wells reports receiving the following, outside the submitted work: personal fees for speaking and for acting on advisory boards from Boehringer Ingelheim, Roche and Bayer.
Figures
Comment in
References
-
- Mikolasch TA, Porter JC. Transbronchial cryobiopsy in the diagnosis of interstitial lung disease: a cool new approach. Respirology 2014; 19: 623–624. - PubMed
-
- Schoenheit G, Becattelli I, Cohen AH. Living with idiopathic pulmonary fibrosis: an in-depth qualitative survey of European patients. Chron Respir Dis 2011; 8: 225–231. - PubMed
-
- Martinez FJ, Collard HR, Pardo A, et al. . Idiopathic pulmonary fibrosis. Nat Rev Dis Primers 2017; 3: 17074. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical