

Detection and Surveillance of Bladder Cancer Using Urine Tumor DNA
- PMID: 30578357
- PMCID: PMC6467650
- DOI: 10.1158/2159-8290.CD-18-0825
Detection and Surveillance of Bladder Cancer Using Urine Tumor DNA
Abstract
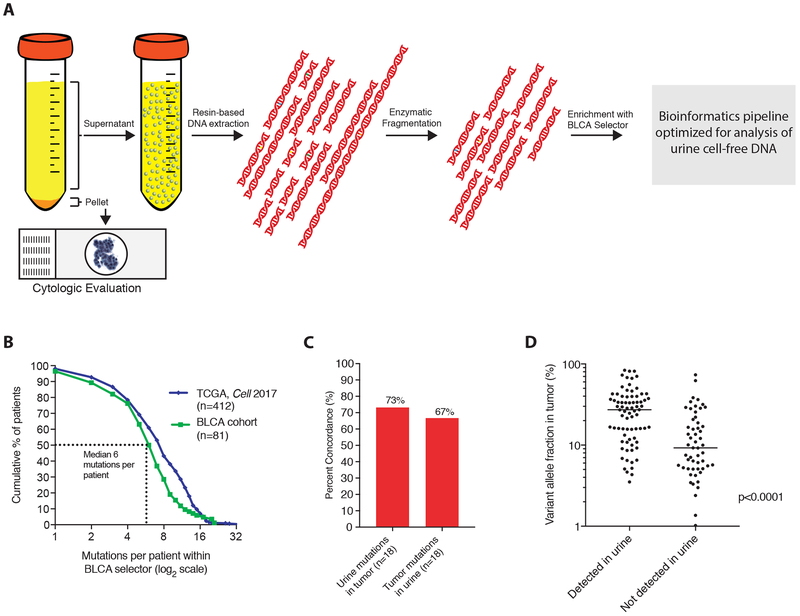
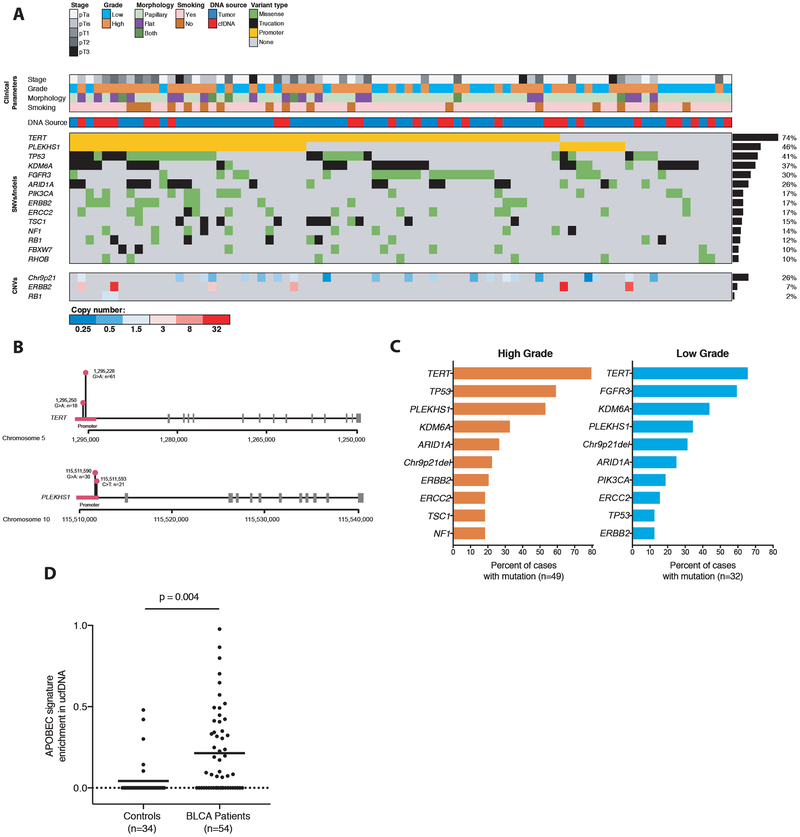
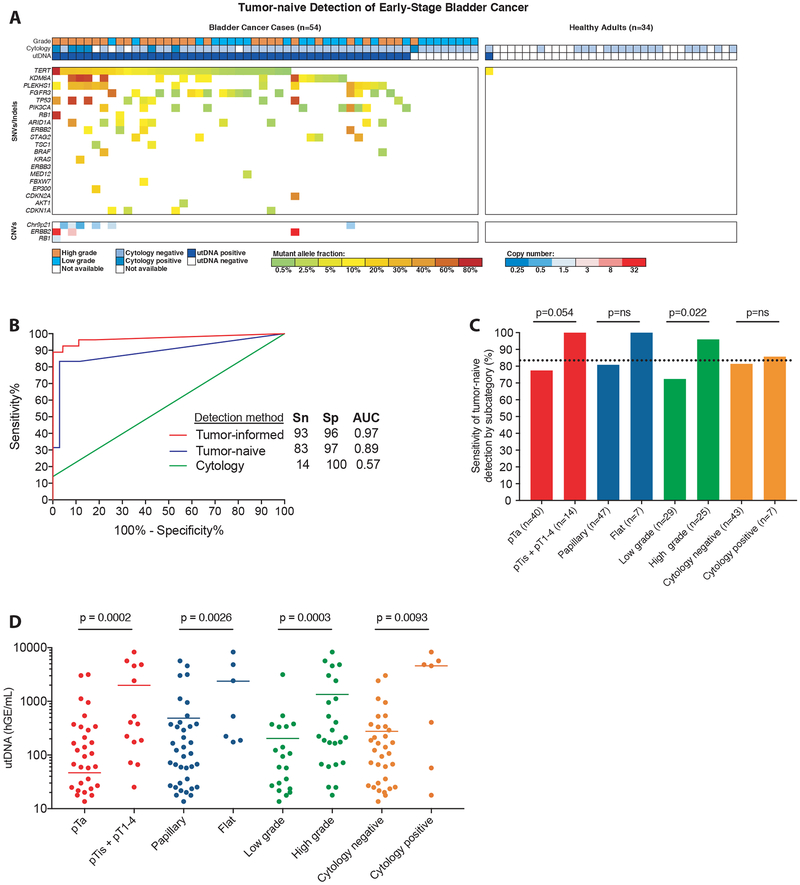
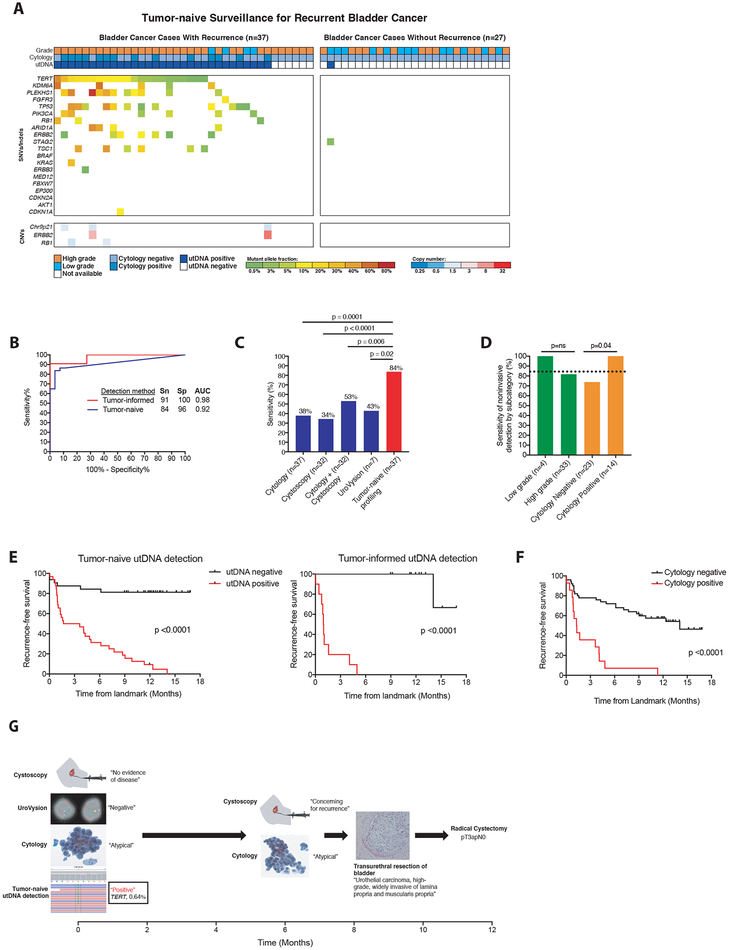
Current regimens for the detection and surveillance of bladder cancer are invasive and have suboptimal sensitivity. Here, we present a novel high-throughput sequencing (HTS) method for detection of urine tumor DNA (utDNA) called utDNA CAPP-Seq (uCAPP-Seq) and apply it to 67 healthy adults and 118 patients with early-stage bladder cancer who had urine collected either prior to treatment or during surveillance. Using this targeted sequencing approach, we detected a median of 6 mutations per patient with bladder cancer and observed surprisingly frequent mutations of the PLEKHS1 promoter (46%), suggesting these mutations represent a useful biomarker for detection of bladder cancer. We detected utDNA pretreatment in 93% of cases using a tumor mutation-informed approach and in 84% when blinded to tumor mutation status, with 96% to 100% specificity. In the surveillance setting, we detected utDNA in 91% of patients who ultimately recurred, with utDNA detection preceding clinical progression in 92% of cases. uCAPP-Seq outperformed a commonly used ancillary test (UroVysion, P = 0.02) and cytology and cystoscopy combined (P ≤ 0.006), detecting 100% of bladder cancer cases detected by cytology and 82% that cytology missed. Our results indicate that uCAPP-Seq is a promising approach for early detection and surveillance of bladder cancer. SIGNIFICANCE: This study shows that utDNA can be detected using HTS with high sensitivity and specificity in patients with early-stage bladder cancer and during post-treatment surveillance, significantly outperforming standard diagnostic modalities and facilitating noninvasive detection, genotyping, and monitoring.This article is highlighted in the In This Issue feature, p. 453.
©2018 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest:
J.D. has served as a consultant for Merck. M.L.Y.S. is an employee at Cepheid. A.A.A. and M.D. are co-inventors on patent applications related to CAPP-Seq. A.A.A. has equity in FortySeven and CiberMed and has served as a consultant for Roche, Genentech, Chugai, and Pharmacyclics. M.D. has equity in CiberMed has served as a consultant for Roche, Novartis, AstraZeneca, Varian Medical Systems, and Quanticel Pharmaceuticals.
Figures
Comment in
-
Massively parallel sequencing of urinary DNA-the dawn of non-invasive bladder cancer detection and surveillance?Transl Cancer Res. 2019 Mar;8(Suppl 2):S204-S207. doi: 10.21037/tcr.2019.03.03. Transl Cancer Res. 2019. PMID: 35117098 Free PMC article. No abstract available.
References
-
- Lotan Y, Roehrborn CG. Sensitivity and specificity of commonly available bladder tumor markers versus cytology: results of a comprehensive literature review and meta-analyses. Urology 2003;61(1):109–18; discussion 18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
