

Evaluation of clinical benefit from treatment with mepolizumab for patients with eosinophilic granulomatosis with polyangiitis
- PMID: 30578883
- PMCID: PMC7254609
- DOI: 10.1016/j.jaci.2018.11.041
Evaluation of clinical benefit from treatment with mepolizumab for patients with eosinophilic granulomatosis with polyangiitis
Erratum in
-
Corrigendum.J Allergy Clin Immunol. 2021 Jun;147(6):2394. doi: 10.1016/j.jaci.2021.03.023. J Allergy Clin Immunol. 2021. PMID: 34092354 No abstract available.
Abstract
Background: In a recent phase III trial (NCT02020889) 53% of mepolizumab-treated versus 19% of placebo-treated patients with eosinophilic granulomatosis with polyangiitis (EGPA) achieved protocol-defined remission.
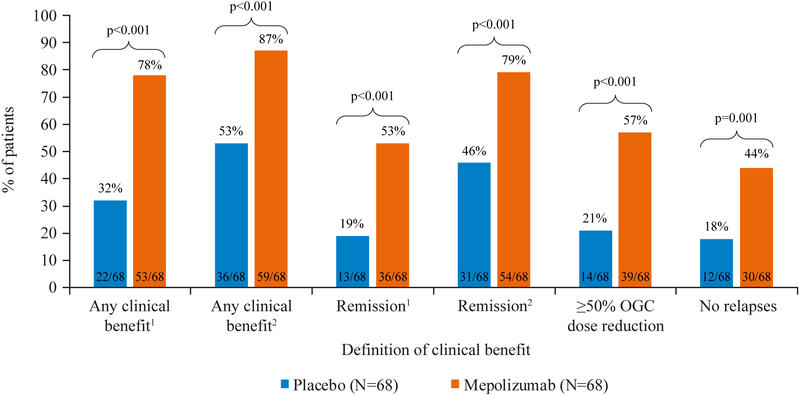
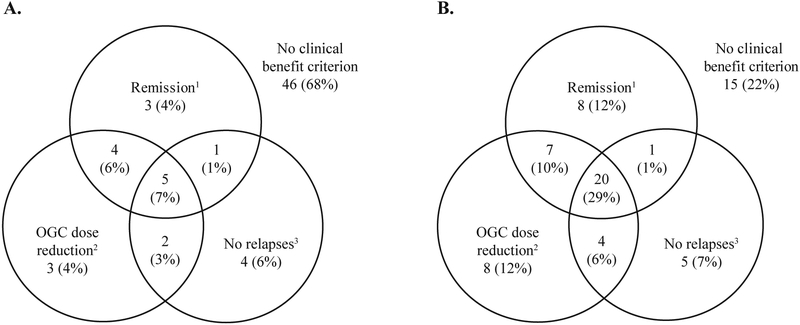
Objective: We sought to investigate post hoc the clinical benefit of mepolizumab in patients with EGPA using a comprehensive definition of benefit encompassing remission, oral glucocorticoid (OGC) dose reduction, and EGPA relapses.
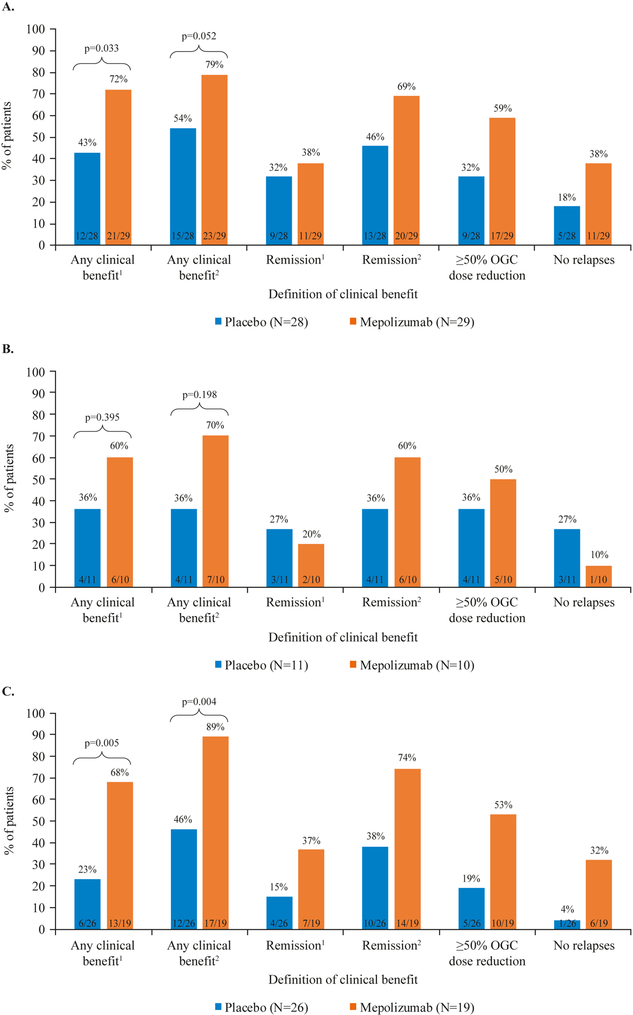
Methods: The randomized, placebo-controlled, double-blind, parallel-group trial recruited patients with relapsing/refractory EGPA receiving stable OGCs (prednisolone/prednisone, ≥7.5-50 mg/d) for 4 or more weeks. Patients received 300 mg of subcutaneous mepolizumab or placebo every 4 weeks for 52 weeks. Clinical benefit was defined post hoc as follows: remission at any time (2 definitions used), 50% or greater OGC dose reduction during weeks 48 to 52, or no EGPA relapses. The 2 remission definitions were Birmingham Vasculitis Activity Score of 0 plus OGC dose of 4 mg/d or less (remission 1/clinical benefit 1) or 7.5 mg/d or less (remission 2/clinical benefit 2). Clinical benefit was assessed in all patients and among subgroups with a baseline blood eosinophil count of less than 150 cells/μL, baseline OGC dosage of greater than 20 mg/d, or weight of greater than 85 kg.
Results: With mepolizumab versus placebo, 78% versus 32% of patients experienced clinical benefit 1, and 87% versus 53% of patients experienced clinical benefit 2 (both P < .001). Significantly more patients experienced clinical benefit 1 with mepolizumab versus placebo in the blood eosinophil count less than 150 cells/μL subgroup (72% vs 43%, P = .033) and weight greater than 85 kg subgroup (68% vs 23%, P = .005); in the OGC greater than 20 mg/d subgroup, results were not significant but favored mepolizumab (60% vs 36%, P = .395).
Conclusion: When a comprehensive definition of clinical benefit was applied to data from a randomized controlled trial, 78% to 87% of patients with EGPA experienced benefit with mepolizumab.
Keywords: Churg-Strauss syndrome; Eosinophilic granulomatosis with polyangiitis; IL-5; eosinophils; mepolizumab; vasculitis.
Copyright © 2018 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest
JS, ESB, JB, SM, and SWY are employees of GSK and own stocks in GSK. PA has received research grants from GSK and the NIH, and has acted as a consultant for Ambrx, GSK, and AstraZeneca. MCC has acted as a consultant for GSK, Novartis, Boehringer Ingelheim, Abbvie and Roche. GJG has received research grants from the NIH, and has acted as a consultant for Genentech. DJ has received research grants from GSK and acted as a consultant for GSK. CAL has received research grants from Bristol-Myers Squibb, Genentech, ChemoCentryx, and GSK and is a non-paid consultant for Bristol-Myers Squibb and Abbvie. PAM has received research funds and/or consulting fees from Abbvie, Actelion, Boehringer Ingelheim, Bristol-Myears Squibb, Celgene, ChemoCentryx, Genentech/Roche, GlaxoSmithKline, InflaRx, Insmed, Kypha, TerumoBCT. FM has received research grants from Roche and has acted as a consultant for Chugai, GSK, Lily, and Roche. MEW has acted as a consultant for AstraZeneca, Boehringer Ingelheim, Boston Scientific, Genentech, GSK, Novartis, Regeneron, Sanofi, Sentien, Teva, and Vectura, and has received research funding from Teva, AstraZeneca, Novartis and Sanofi. PFW has received research grants from NIH and acted as a consultant for GSK. PK and US have no conflicts of interest to declare.
Figures
Comment in
-
Mepolizumab in patients with eosinophilic granulomatosis with polyangiitis.J Allergy Clin Immunol. 2019 Aug;144(2):621. doi: 10.1016/j.jaci.2019.03.030. Epub 2019 May 2. J Allergy Clin Immunol. 2019. PMID: 31056188 No abstract available.
-
Reply.J Allergy Clin Immunol. 2019 Aug;144(2):622. doi: 10.1016/j.jaci.2019.03.031. Epub 2019 May 2. J Allergy Clin Immunol. 2019. PMID: 31056189 No abstract available.
References
-
- Vaglio A, Buzio C, Zwerina J. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): state of the art. Allergy. 2013;68(3):261–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
