

Rhombencephalosynapsis: Fused cerebellum, confused geneticists
- PMID: 30580482
- PMCID: PMC6540982
- DOI: 10.1002/ajmg.c.31666
Rhombencephalosynapsis: Fused cerebellum, confused geneticists
Abstract
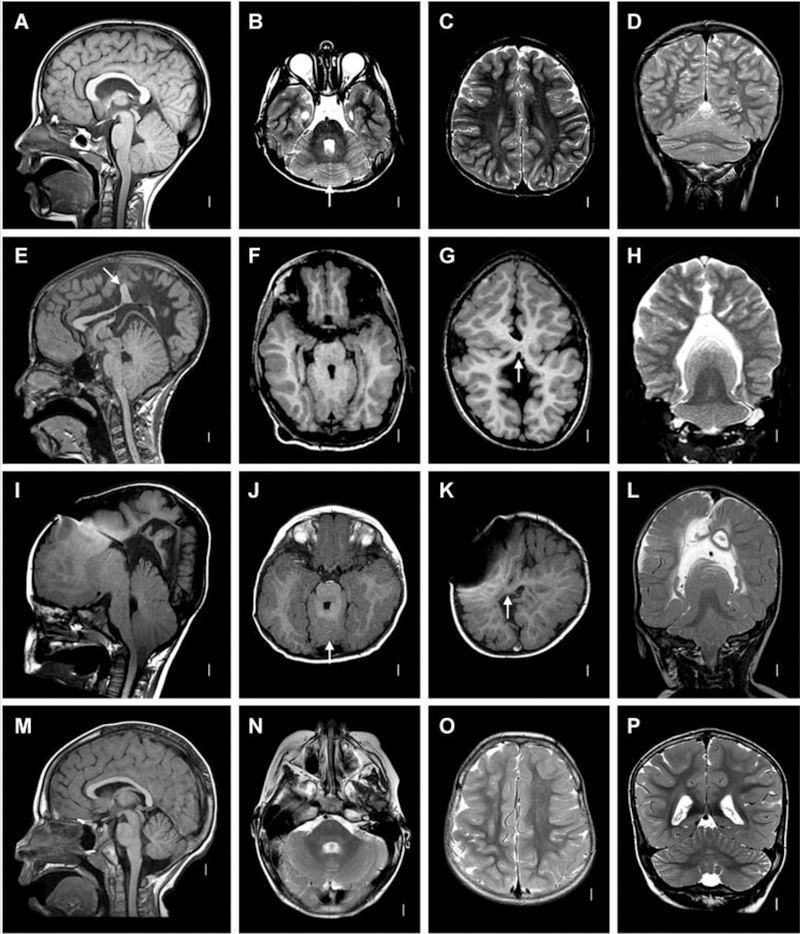
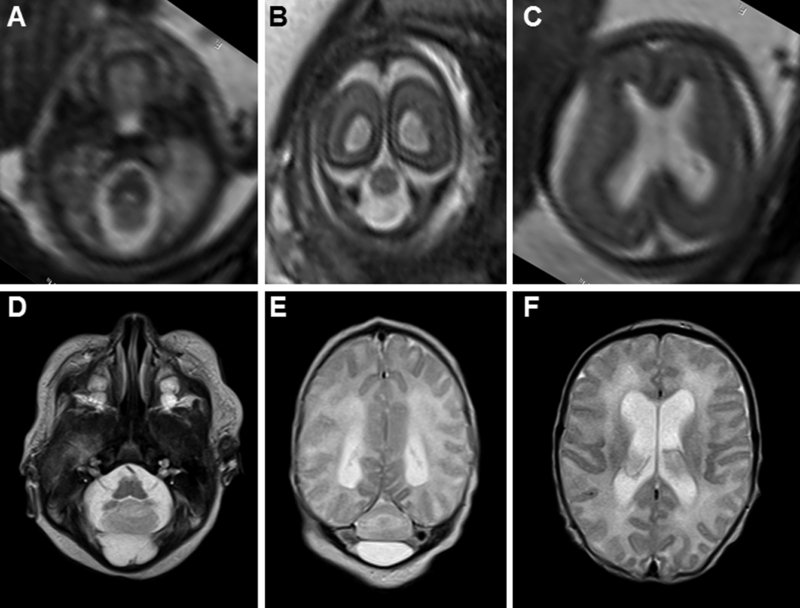
Rhombencephalosynapsis (RES) is a unique cerebellar malformation characterized by fusion of the cerebellar hemispheres with partial or complete absence of a recognizable cerebellar vermis. Subsets of patients also have other brain malformations such as midbrain fusion with aqueductal stenosis, characteristic craniofacial features (prominent forehead, flat midface, hypertelorism, ear abnormalities), and somatic malformations (heart, kidney, spine, and limb defects). Similar to known genetic brain malformations, the RES cerebellar malformation is highly stereotyped, yet no genetic causes have been identified. Here, we outline our current understanding of the genetic basis for RES, discuss limitations, and outline future approaches to identifying the causes of this fascinating brain malformation.
Keywords: RES; cerebellum; genetics; neuroimaging.
© 2018 Wiley Periodicals, Inc.
Figures

References
-
- de Mattos VF, Graziadio C, Machado Rosa RF, Lenhardt R, Alves RP, Trevisan P, . . . Zen PR (2014). Gomez-Lopez-Hernandez syndrome in a child born to consanguineous parents: new evidence for an autosomal-recessive pattern of inheritance? Pediatr Neurol, 50(6), 612–615. doi: 10.1016/j.pediatrneurol.2014.01.035 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
