

Hypoperfusion Symptoms Poorly Predict Hemodynamic Compromise and Stroke Risk in Vertebrobasilar Disease
- PMID: 30580717
- PMCID: PMC6349517
- DOI: 10.1161/STROKEAHA.118.023101
Hypoperfusion Symptoms Poorly Predict Hemodynamic Compromise and Stroke Risk in Vertebrobasilar Disease
Abstract
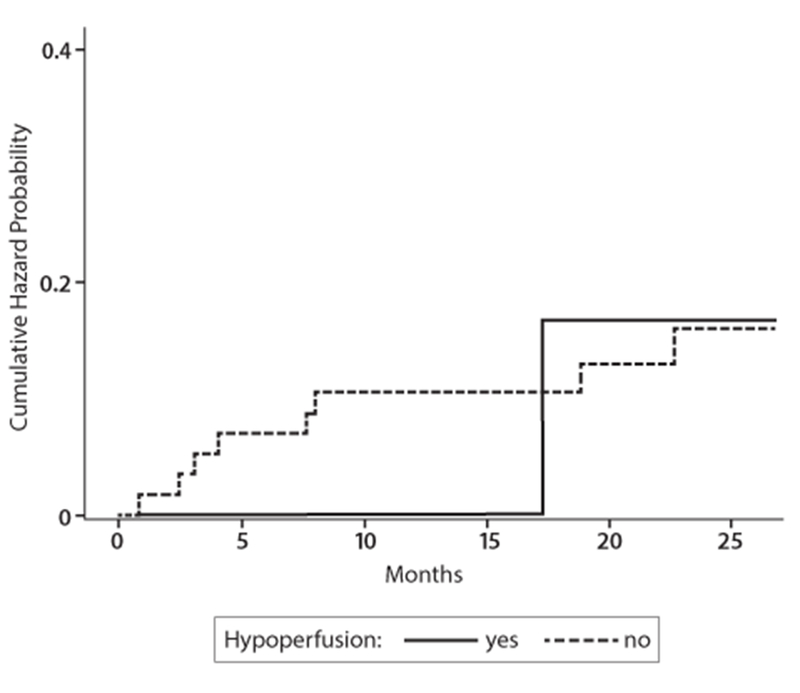
Background and Purpose- Cerebral hypoperfusion symptoms (defined as symptoms related to change in position, effort or exertion, or recent change in antihypertensive medication) have been used in stroke studies as a surrogate for detecting hemodynamic compromise. However, the validity of these symptoms in identifying flow compromise in patients has not been well established. We examined whether hypoperfusion symptoms correlated with quantitative measurements of flow compromise in the prospective, observational VERiTAS study (Vertebrobasilar Flow Evaluation and Risk of Transient Ischemic Attack and Stroke). Methods- VERiTAS enrolled patients with recent vertebrobasilar transient ischemic attack or stroke and ≥50% atherosclerotic stenosis or occlusion in vertebral or basilar arteries. Hemodynamic status using vertebrobasilar large vessel flow was measured using quantitative magnetic resonance angiography, and patients were designated as low, borderline, or normal flow based on distal territory regional flow, incorporating collateral capacity. The presence of qualifying event hypoperfusion symptoms was assessed relative to the quantitatively determined flow status (normal versus borderline/low) and also examined as a predictor of subsequent stroke risk. Results- Of the 72 enrolled subjects, 66 had data on hypoperfusion symptoms available. On initial quantitative magnetic resonance angiography designation, 43 subjects were designated as normal flow versus 23 subjects designated as low flow (n=16) or borderline flow (n=7). Of these, 5 (11.6%) normal flow and 3 (13.0%) low/borderline flow subjects reported at least one qualifying event hypoperfusion symptom ( P=0.99, Fisher exact test). Hypoperfusion symptoms had a positive predictive value of 37.5% and negative predictive value of 65.5% for low/borderline flow status. Compared with flow status, which strongly predicted subsequent stroke risk, hypoperfusion symptoms were not associated with stroke outcome ( P=0.87, log-rank test). Conclusions- These results suggest that hypoperfusion symptoms alone correlate poorly with actual hemodynamic compromise as assessed by quantitative magnetic resonance angiography and subsequent stroke risk in vertebrobasilar disease, and are not a reliable surrogate for flow measurement. Clinical Trial Registration- URL: https://www.clinicaltrials.gov . Unique identifier: NCT00590980.
Keywords: hemodynamics; magnetic resonance angiography; magnetic resonance imaging; risk; stroke; vertebrobasilar ischemia.
Conflict of interest statement
CONFLICTS OF INTEREST/DISCLOSURES
PBG: consultant Brainsgate, NeuroSpring
Figures

References
-
- Grubb RL, Derdeyn CP, Fritsch SM, Carpenter DA, Yundt KD, Videen TO, et al. Importance of hemodynamic factors in the prognosis of symptomatic carotid occlusion. JAMA. 1998;280:1055–1060 - PubMed
-
- Mazighi M, Tanasescu R, Ducrocq X, Vicaut E, Bracard S, Houdart E, et al. Prospective study of symptomatic atherothrombotic intracranial stenoses: The gesica study. Neurology. 2006;66:1187–1191 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
