

Papillary muscles of left ventricle-Morphological variations and it's clinical relevance
- PMID: 30580862
- PMCID: PMC6306352
- DOI: 10.1016/j.ihj.2017.12.003
Papillary muscles of left ventricle-Morphological variations and it's clinical relevance
Abstract
Introduction: The two left ventricular papillary muscles are small structures at sternocostal and inferior wall but are vital to mitral valve competence. Extra papillary muscles could be found. Partial or complete rupture, complicating acute myocardial infarction, causes severe or even catastrophic mitral regurgitation, potentially correctable by surgery. Detailed knowledge of normal anatomy and variations is vital for accurate interpretation of information by echocardiography and for surgical repair.
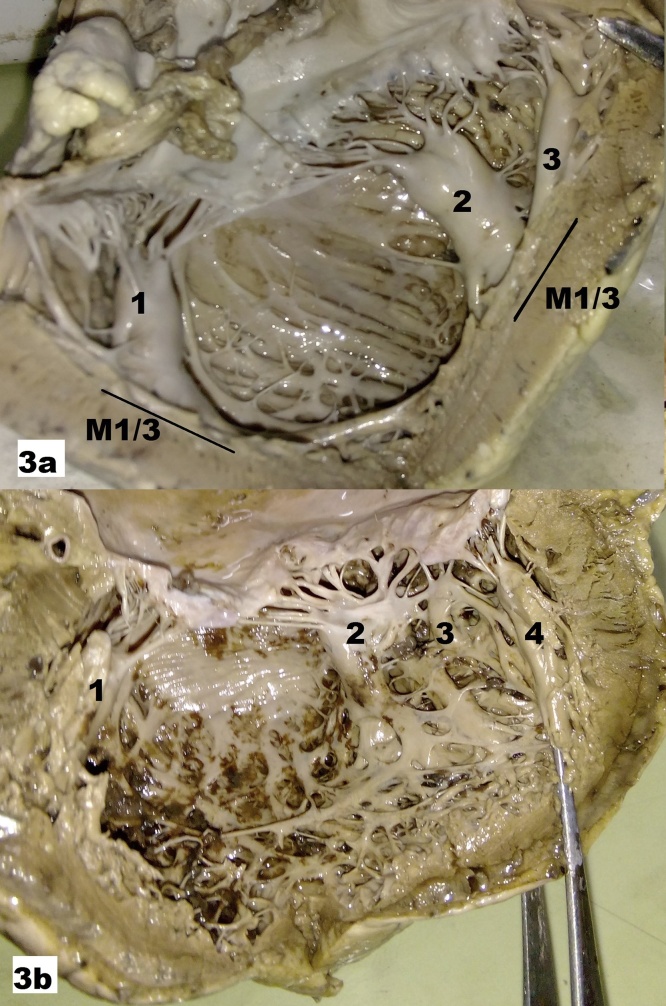
Materials and methods: The material for present study consisted of 52 formalin fixed adult apparently normal cadaveric hearts belonging to either sex obtained from the Department of Anatomy. These hearts were dissected carefully to open the left ventricle and to expose the papillary muscles. According to their attitudinal position they were described as supero-lateral (S-L) and inferoseptal muscle (I-S) instead of conventional anterolateral and posteromedial. Different morphological features of papillary muscles were noted and measurements were taken.
Results: Classical picture of left ventricular papillary muscle was found only in 25% cases. Additionally extra muscles were found 34.61% and 71.15% in S-L and I-S group, respectively. Different shapes and pattern of papillary muscles were also been identified. An additional attribute of this study was measurement of length and breadth of papillary muscles which thus provides a base line data for further detailed studies in a large scale.
Conclusion: Oriental nomenclature is necessary not only for anatomist but also for electrocardiographers. Breadth of papillay muscle should be taken into morphometric account as for screening of hypertrophic cardiomyopathy. Proper anatomical knowledge is crucial for clinicians, surgeons and radiologists.
Keywords: Heart; Left ventricle; Mitral valve; Papillary muscles.
Copyright © 2017 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
Figures





References
-
- Anderson R.H. The relationship between the positions of the left ventricular papillary muscles and the direction of the QRS axis. J Electrophysiol Cardiol. 2016;49(5):675–679. - PubMed
-
- Mittal A.K., Langston M., Cohn K.E., Selzer A., Kerth W.J. Combined papillary muscle and left ventricular wall dysfunction as a cause of mitral regurgitation. Circulation. 1971;44:174–180. - PubMed
-
- Madu E.C., Baugh D.S., Reid E.C., Potu C. Papillary muscle function does not predict mitral regurgitation in patients with normal left ventricular systolic function: a transesophageal echocardiographic study − PM function and mitral regurgitation. Inter J Clin Med. 2011;2:178–183.
MeSH terms
LinkOut - more resources
Full Text Sources
