

5-HTTLPR and MTHFR 677C>T polymorphisms and response to yoga-based lifestyle intervention in major depressive disorder: A randomized active-controlled trial
- PMID: 30581206
- PMCID: PMC6278208
- DOI: 10.4103/psychiatry.IndianJPsychiatry_398_17
5-HTTLPR and MTHFR 677C>T polymorphisms and response to yoga-based lifestyle intervention in major depressive disorder: A randomized active-controlled trial
Abstract
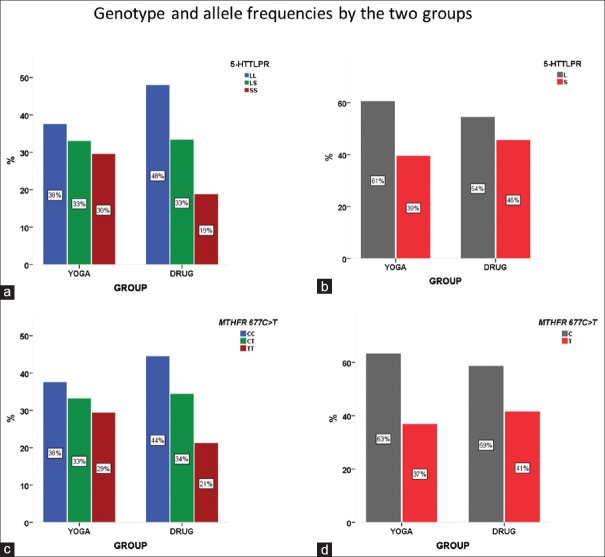
Background: There is growing evidence suggesting that both genetic and environmental factors modulate treatment outcome in, a highly heterogeneous, major depressive disorder (MDD). 5-HTTLPR variant of the serotonin transporter gene (SLC6A4) and MTHFR 677C>T polymorphisms have been linked to the pathogenesis of MDD, and antidepressant treatment response. The evidence is lacking on the clinical utility of yoga in patients with MDD who have 5-HTTLPR and MTHFR 677C>T polymorphisms and less likely to respond to medications (SSRIs).
Aims: We aimed to examine the impact of YBLI in those who have susceptible 5-HTTLPR and MTHFR 677C>T polymorphisms and are less likely to drug therapy with SSRIs.
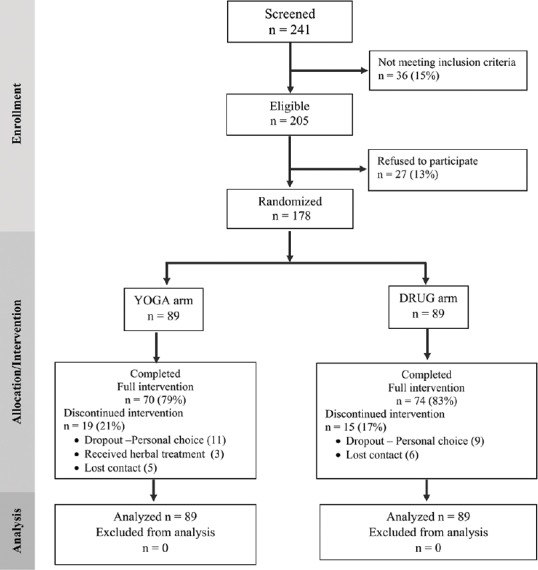
Settings and design: In a 12 week randomized active-controlled trial, MDD patients (n = 178) were randomized to receive YBLI or drug therapy.
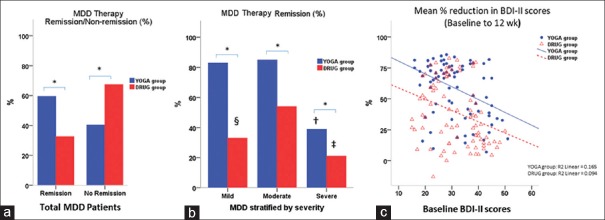
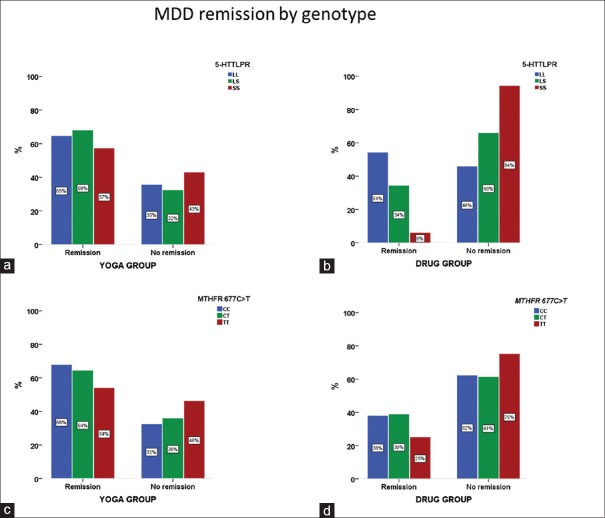
Methods: Genotyping was conducted using PCR-based methods. The clinical remission was defined as BDI-II score ≤ 9.
Statistical analysis used: An intent-to-treat analysis was performed, and the association of genotype with treatment remission consisted of the logistic regression model. A P value of <0.05 was considered statistically significant.
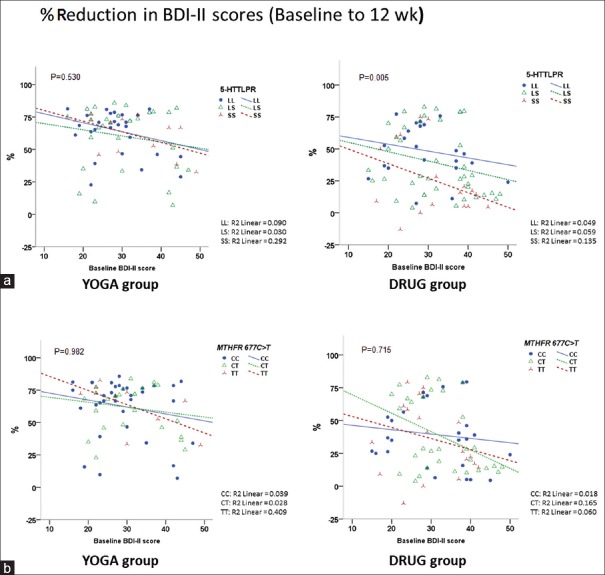
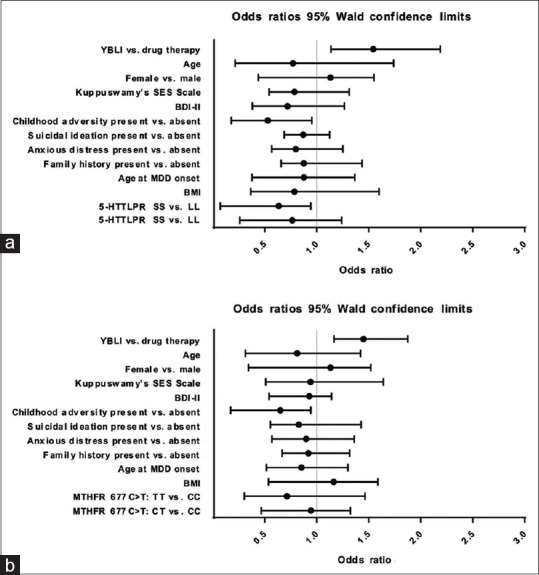
Results: Multivariate logistic regression models for remission including either 5-HTTLPR or MTHFR 677C>T genotypes showed statistically significant odds of remission in YOGA arm vs. DRUG arm. Neither 5-HTTLPR nor MTHFR 677C>T genotype showed any influence on remission to YBLI (P = 0.73 and P = 0.64, respectively). Further analysis showed childhood adversity interact with 5-HTTLPR and MTHFR 677C>T polymorphisms to decrease treatment response in DRUG treatment arm, but not in YOGA arm.
Conclusions: YBLI provides MDD remission in those who have susceptible 5-HTTLPR and MTHFR 677C>T polymorphisms and are resistant to SSRIs treatment. YBLI may be therapeutic for MDD independent of heterogeneity in its etiopathogenesis.
Keywords: 5-HTTLPR; MTHFR 677C>T; depression; gene-environment; meditation; yoga.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- World Health Organization. Geneva: World Health Organization; 2017. [Last accessed on 2018 Jan 11]. Depression and Other Common Mental Disorders: Global Health Estimates. Available from: http://www.apps.who.int/iris/handle/10665/254610 .
-
- Verhoeven JE, Révész D, Epel ES, Lin J, Wolkowitz OM, Penninx BW. Major depressive disorder and accelerated cellular aging: Results from a large psychiatric cohort study. Mol Psychiatry. 2014;19:895–901. - PubMed
-
- Baldessarini RJ, Forte A, Selle V, Sim K, Tondo L, Undurraga J, et al. Morbidity in depressive disorders. Psychother Psychosom. 2017;86:65–72. - PubMed
-
- Otte C, Gold SM, Penninx BW, Pariante CM, Etkin A, Fava M, et al. Major depressive disorder. Nat Rev Dis Primers. 2016;2:16065. - PubMed
