

Is there a role for reproductive steroids in the etiology and treatment of affective disorders?
- PMID: 30581288
- PMCID: PMC6296393
- DOI: 10.31887/DCNS.2018.20.3/drubinow
Is there a role for reproductive steroids in the etiology and treatment of affective disorders?
Abstract
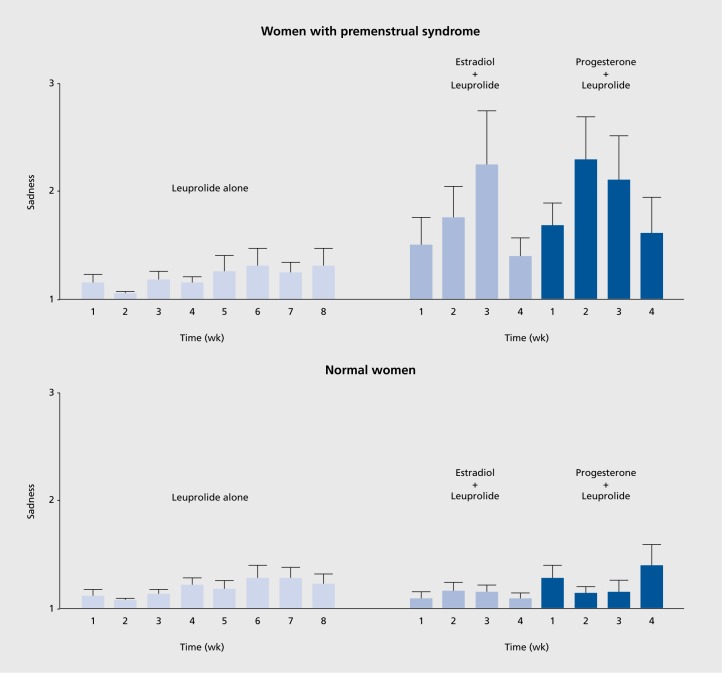
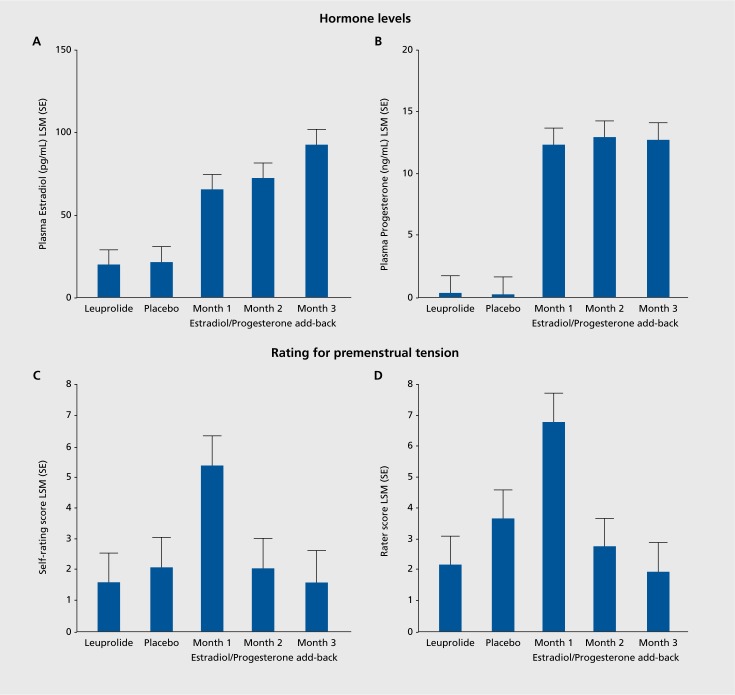
A variety of hormones have been shown to play a role in affective disorders. Reproductive steroids are particularly informative in our efforts to understand the pathophysiology of affective dysregulation for several reasons: i) Reproductive endocrine-related mood disorders (premenstrual dysphoric disorder, perinatal depression, perimenopausal depression) are wonderful clinical models for investigating the mechanisms by which affective state changes occur; ii) Reproductive steroids regulate virtually every system that has been implicated as disturbed in the ontogeny of affective disorders; iii) Despite the absence of a reproductive endocrinopathy a triggering role in the affective disturbance of reproductive mood disorders has been shown clearly for changes in reproductive steroids. The existing data, therefore, support a differential sensitivity to reproductive steroids in reproductive mood disorders such that an abnormal affective state is precipitated by normal changes in reproductive steroids. The therapeutic implications of these findings for affective illness are discussed.
Se ha demostrado que diversas hormonas desempeñan un papel en los trastornos afectivos. Los esteroides sexuales han aportado importante información en nuestros esfuerzos por comprender la fisiopatología de la desregulación afectiva por varias razones: 1) Los trastornos del estado de ánimo relacionados con el sistema endocrino reproductivo (trastorno disfórico premenstrual, depresión perinatal, depresión perimenopáusica) son excelentes modelos clínicos para investigar los mecanismos por los cuales se producen cambios en el estado afectivo, 2) Los esteroides sexuales regulan virtualmente todos los sistemas que se han involucrado en las alteraciones de la ontogenia de los trastornos afectivos y 3) A pesar de la ausencia de una endocrinopatía reproductiva, se ha demostrado claramente que los cambios en los esteroides sexuales tienen un papel desencadenante en la alteración afectiva de los trastornos del estado de ánimo reproductivo. Por lo tanto, los datos existentes apoyan una sensibilidad diferencial a los esteroides sexuales en los trastornos del estado de ánimo reproductivo, de manera que los cambios normales en los esteroides sexuales precipitan un estado afectivo anormal. Se discuten las consecuencias terapéuticas de estos hallazgos para la enfermedad afectiva.
Il a été prouvé que certaines hormones jouent un rôle dans les troubles de l'humeur. Les hormones sexuelles nous ont particulièrement instruits dans notre démarche pour comprendre la physiopathologie de la dysrégulation de l'humeur pour plusieurs raisons : 1) les troubles de l'humeur liés au système endocrinien sexuel (trouble dysphorique prémenstruel, dépression périnatale, dépression périménopausique) sont de parfaits modèles cliniques pour la recherche des mécanismes sous-jacents aux changements d'humeur ; 2) les stéroïdes sexuels régulent pratiquement tout système ayant été identifié comme perturbé dans l'ontogenèse des troubles de l'humeur ; 3) Même en l'absence de pathologie endocrinienne, les variations de taux de stéroïdes sexuels ont clairement démontré le rôle déclencheur des perturbations liées à la reproduction dans les troubles de l'humeur. Les données existantes sont donc en faveur d'une sensibilité différentielle aux stéroïdes sexuels dans les troubles de l'humeur liés à la reproduction telle qu'un état émotionnel anormal est déclenché par des variations normales de stéroïdes sexuels. Nous discuterons des implications thérapeutiques de ces résultats pour les troubles de l'humeur.
Keywords: PMDD; affect; depression; hormone; reproductive steroid.
Figures
Similar articles
-
Reproductive Steroid Regulation of Mood and Behavior.Compr Physiol. 2016 Jun 13;6(3):1135-60. doi: 10.1002/cphy.c150014. Compr Physiol. 2016. PMID: 27347888 Free PMC article. Review.
-
Allopregnanolone as a mediator of affective switching in reproductive mood disorders.Psychopharmacology (Berl). 2014 Sep;231(17):3557-67. doi: 10.1007/s00213-014-3599-x. Epub 2014 May 21. Psychopharmacology (Berl). 2014. PMID: 24846476 Free PMC article. Review.
-
The ESC/E(Z) complex, an effector of response to ovarian steroids, manifests an intrinsic difference in cells from women with premenstrual dysphoric disorder.Mol Psychiatry. 2017 Aug;22(8):1172-1184. doi: 10.1038/mp.2016.229. Epub 2017 Jan 3. Mol Psychiatry. 2017. PMID: 28044059 Free PMC article.
-
Premenstrual Dysphoric Disorder: Epidemiology and Treatment.Curr Psychiatry Rep. 2015 Nov;17(11):87. doi: 10.1007/s11920-015-0628-3. Curr Psychiatry Rep. 2015. PMID: 26377947 Free PMC article. Review.
-
The clinical nature and formal diagnosis of premenstrual, postpartum, and perimenopausal affective disorders.Curr Psychiatry Rep. 2002 Dec;4(6):419-28. doi: 10.1007/s11920-002-0069-7. Curr Psychiatry Rep. 2002. PMID: 12441021 Review.
Cited by
-
Age- and sex-specific effects of stress on parvalbumin interneurons in preclinical models: Relevance to sex differences in clinical neuropsychiatric and neurodevelopmental disorders.Neurosci Biobehav Rev. 2021 Dec;131:1228-1242. doi: 10.1016/j.neubiorev.2021.10.031. Epub 2021 Oct 27. Neurosci Biobehav Rev. 2021. PMID: 34718048 Free PMC article. Review.
-
What Pre-clinical Rat Models Can Tell Us About Anxiety Across the Menstrual Cycle in Healthy and Clinically Anxious Humans.Curr Psychiatry Rep. 2022 Nov;24(11):697-707. doi: 10.1007/s11920-022-01376-7. Epub 2022 Oct 18. Curr Psychiatry Rep. 2022. PMID: 36255558 Free PMC article. Review.
-
The Influence of Running and Dancing on the Occurrence and Progression of Premenstrual Disorders.Int J Environ Res Public Health. 2021 Jul 27;18(15):7946. doi: 10.3390/ijerph18157946. Int J Environ Res Public Health. 2021. PMID: 34360242 Free PMC article.
-
Pubertal development and risk of premenstrual disorders in young adulthood.Hum Reprod. 2021 Jan 25;36(2):455-464. doi: 10.1093/humrep/deaa309. Hum Reprod. 2021. PMID: 33289027 Free PMC article.
-
Participation of the Serotonergic System and Brain-Derived Neurotrophic Factor in the Antidepressant-like Effect of Flavonoids.Int J Mol Sci. 2022 Sep 17;23(18):10896. doi: 10.3390/ijms231810896. Int J Mol Sci. 2022. PMID: 36142808 Free PMC article. Review.
References
-
- Forbes TR. A. A. Berthold and the first endocrine experiment: Some speculations as to its origin. Bull Hist Med. 1949;23:263–267. - PubMed
-
- Borell M. Brown-Séquard's organotherapy and its appearance in America at the end of the nineteenth century. Bull Hist Med. 1976;50(3):309–320. - PubMed
-
- Starling EH. The Croonian lectures on the chemical correlation of the functions of the body. Lancet. 1905;166(4275):339–341.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical