

Tissue Resident CCR2- and CCR2+ Cardiac Macrophages Differentially Orchestrate Monocyte Recruitment and Fate Specification Following Myocardial Injury
- PMID: 30582448
- PMCID: PMC6626616
- DOI: 10.1161/CIRCRESAHA.118.314028
Tissue Resident CCR2- and CCR2+ Cardiac Macrophages Differentially Orchestrate Monocyte Recruitment and Fate Specification Following Myocardial Injury
Abstract
Rationale: Recent advancements have brought to light the origins, complexity, and functions of tissue-resident macrophages. However, in the context of tissue injury or disease, large numbers of monocytes infiltrate the heart and are thought to contribute to adverse remodeling and heart failure pathogenesis. Little is understood about the diversity of monocytes and monocyte-derived macrophages recruited to the heart after myocardial injury, including the mechanisms that regulate monocyte recruitment and fate specification.
Objective: We sought to test the hypothesis that distinct subsets of tissue-resident CCR2- (C-C chemokine receptor 2) and CCR2+ macrophages orchestrate monocyte recruitment and fate specification after myocardial injury.
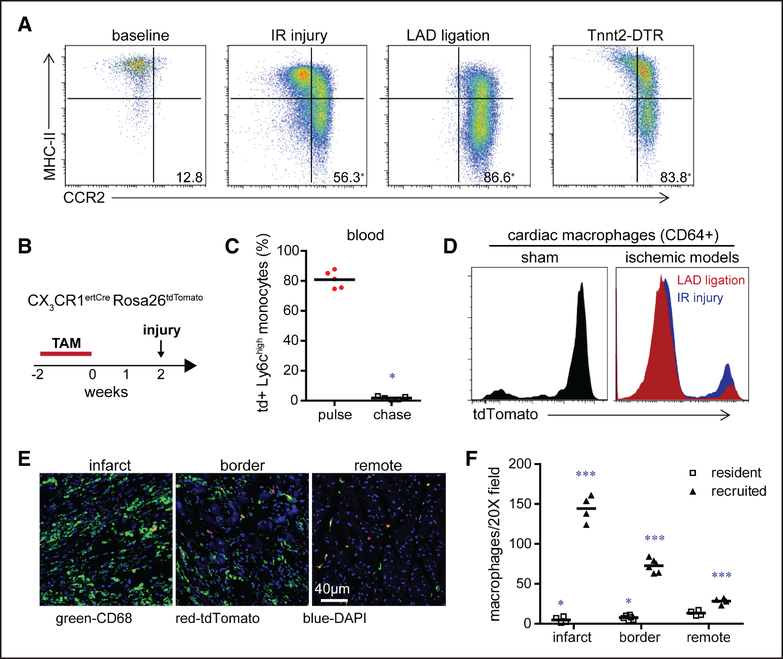
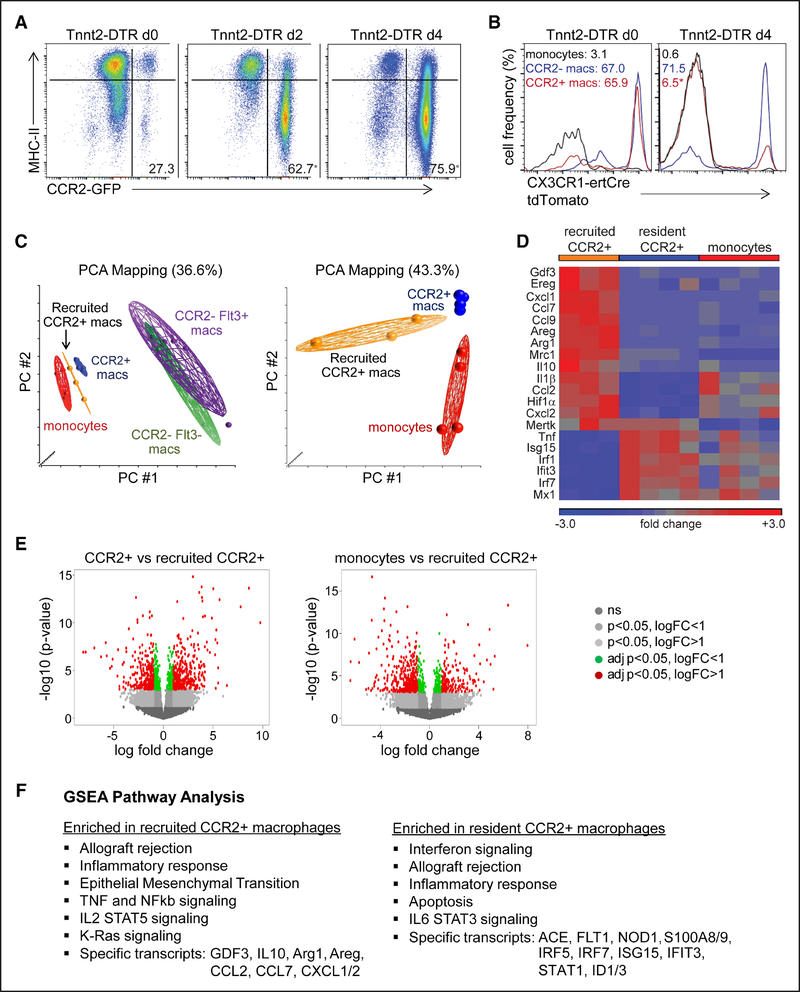
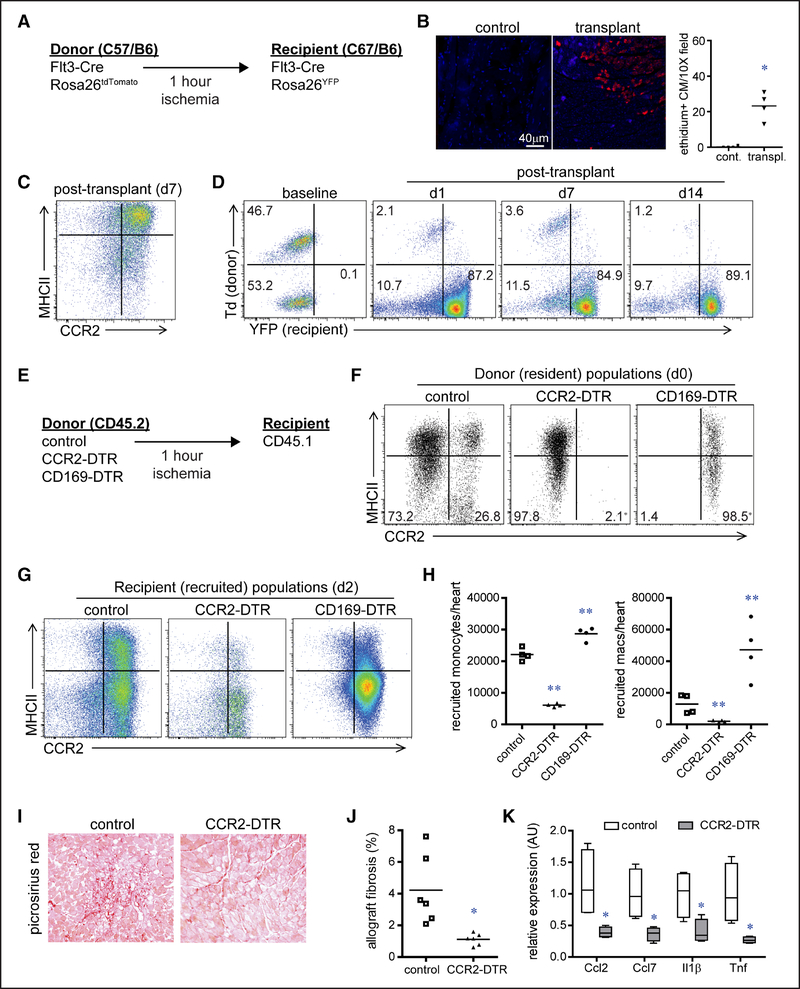
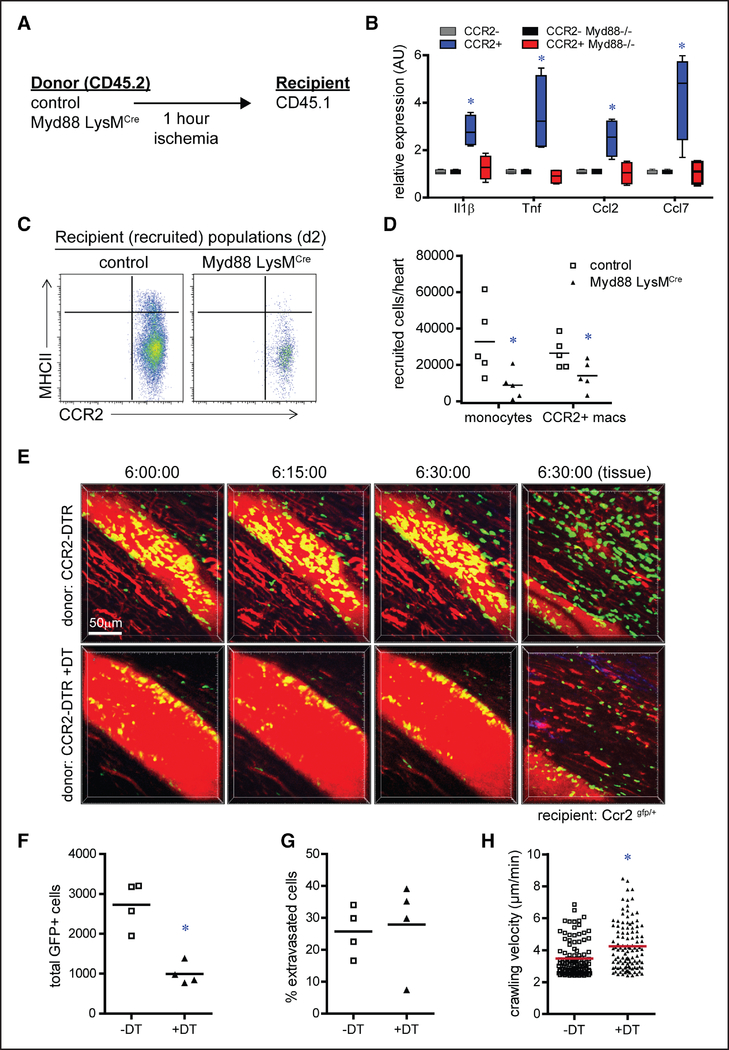
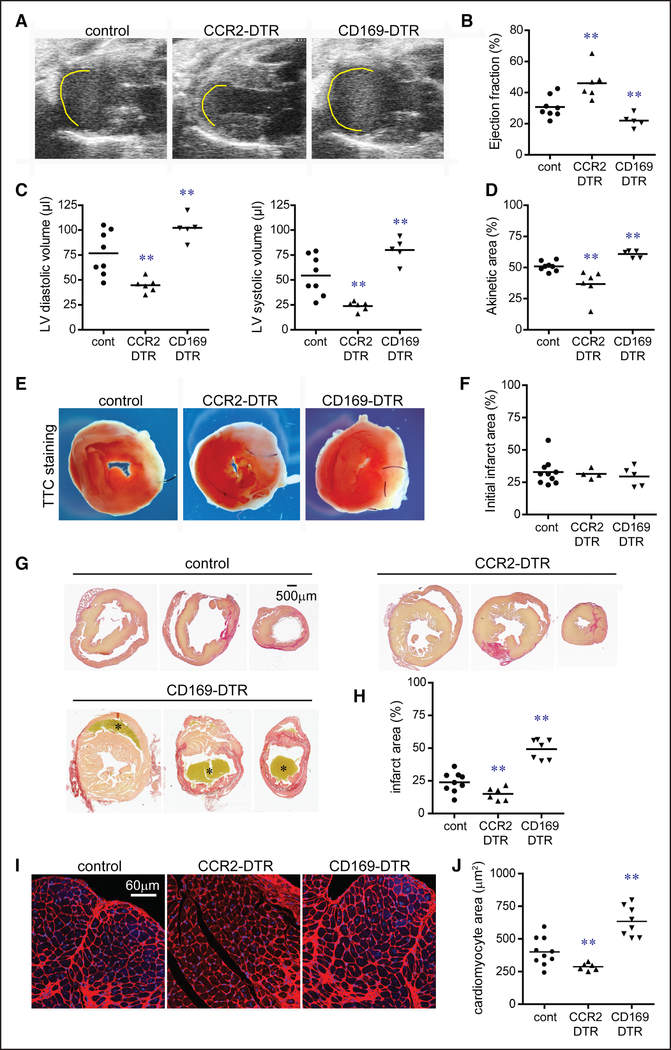
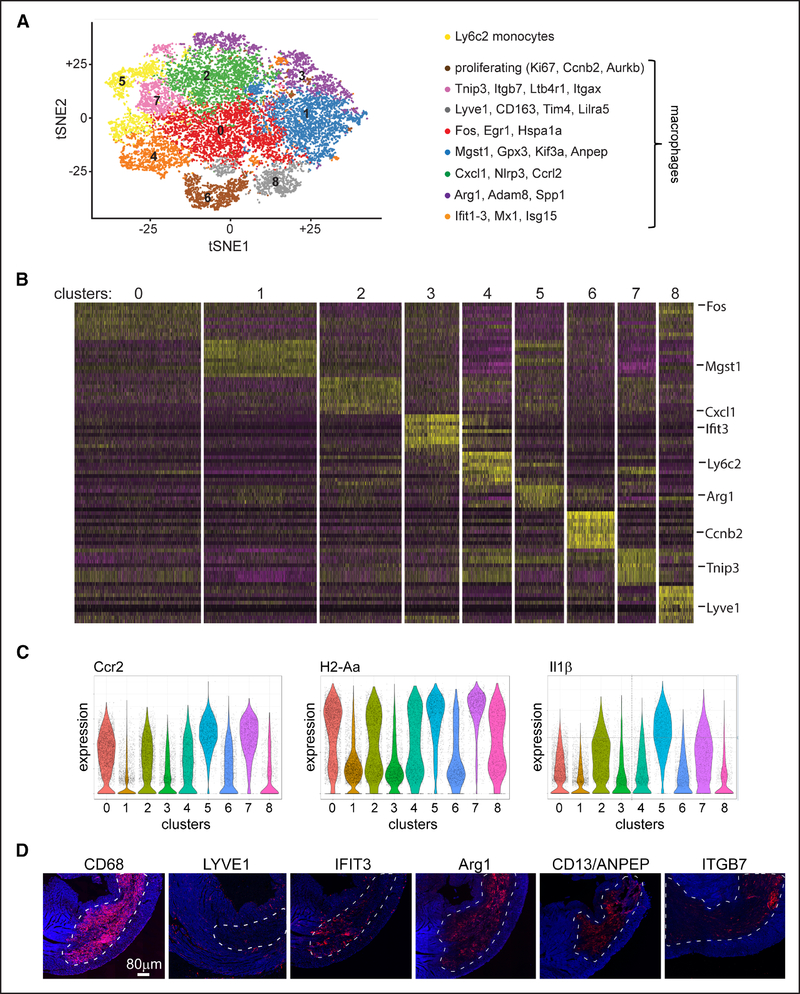
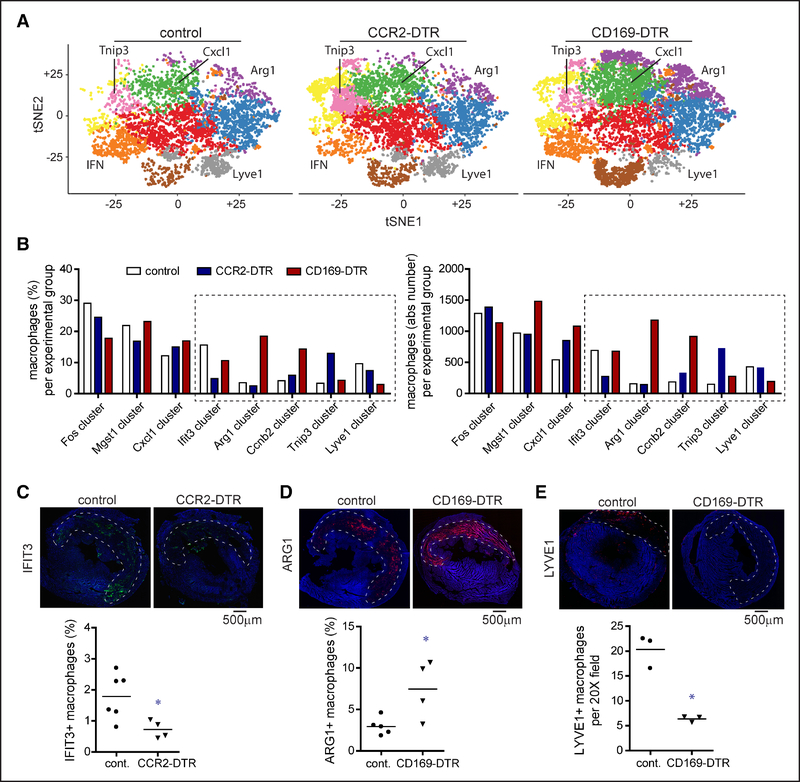
Methods and results: We reveal that in numerous mouse models of cardiomyocyte cell death (permanent myocardial infarction, reperfused myocardial infarction, and diphtheria toxin cardiomyocyte ablation), there is a shift in macrophage ontogeny whereby tissue-resident macrophages are predominately replaced by infiltrating monocytes and monocyte-derived macrophages. Using syngeneic cardiac transplantation to model ischemia-reperfusion injury and distinguish tissue-resident from recruited cell populations in combination with intravital 2-photon microscopy, we demonstrate that monocyte recruitment is differentially orchestrated by distinct subsets of tissue-resident cardiac macrophages. Tissue-resident CCR2+ macrophages promote monocyte recruitment through an MYD88 (myeloid differentiation primary response 88)-dependent mechanism that results in release of MCPs (monocyte chemoattractant proteins) and monocyte mobilization. In contrast, tissue-resident CCR2- macrophages inhibit monocyte recruitment. Using CD (cluster of differentiation) 169-DTR (diphtheria toxin receptor) and CCR2-DTR mice, we further show that selective depletion of either tissue-resident CCR2- or CCR2+ macrophages before myocardial infarction results in divergent effects on left ventricular function, myocardial remodeling, and monocyte recruitment. Finally, using single-cell RNA sequencing, we show that tissue-resident cardiac macrophages differentially instruct monocyte fate specification.
Conclusions: Collectively, these observations establish the mechanistic basis by which monocytes are initially recruited to the injured heart and provide new insights into the heterogeneity of monocyte-derived macrophages.
Keywords: inflammation; macrophages; monocytes; myocardial infarction; receptors, CCR2.
Figures
Comment in
-
The Functional Heterogeneity of Resident Cardiac Macrophages in Myocardial InjuryCCR2+ Cells Promote Inflammation, Whereas CCR2- Cells Protect.Circ Res. 2019 Jan 18;124(2):183-185. doi: 10.1161/CIRCRESAHA.118.314357. Circ Res. 2019. PMID: 30653429 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
