Extracellular Vesicles: New Players in Lymphomas
- PMID: 30583481
- PMCID: PMC6337615
- DOI: 10.3390/ijms20010041
Extracellular Vesicles: New Players in Lymphomas
Abstract
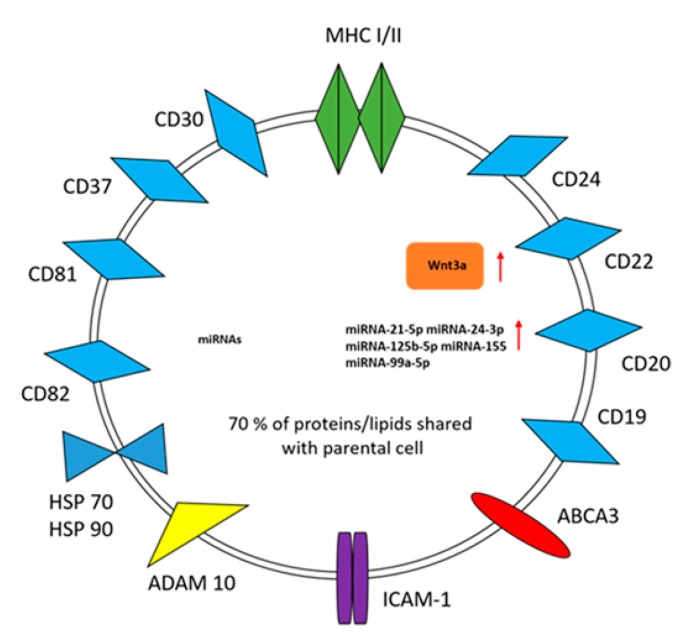
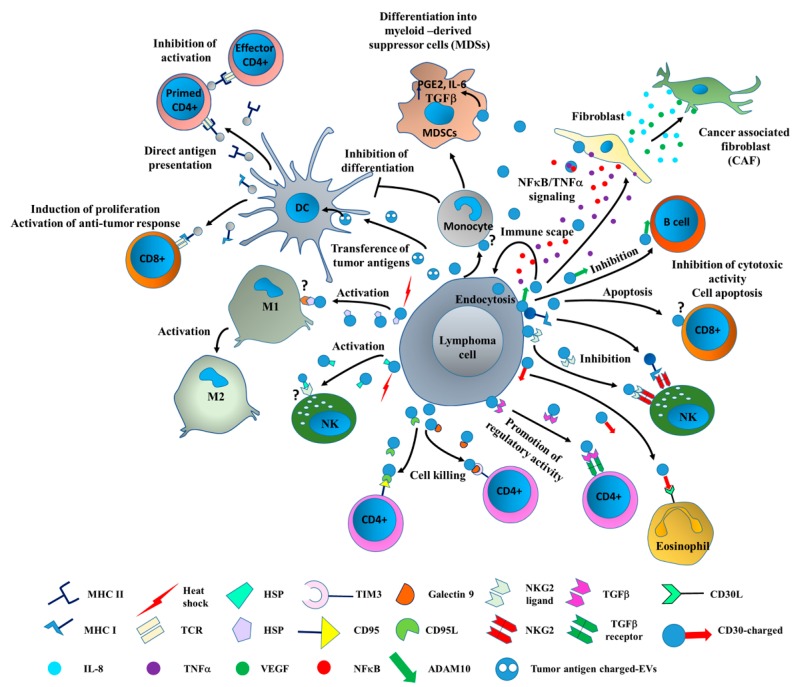
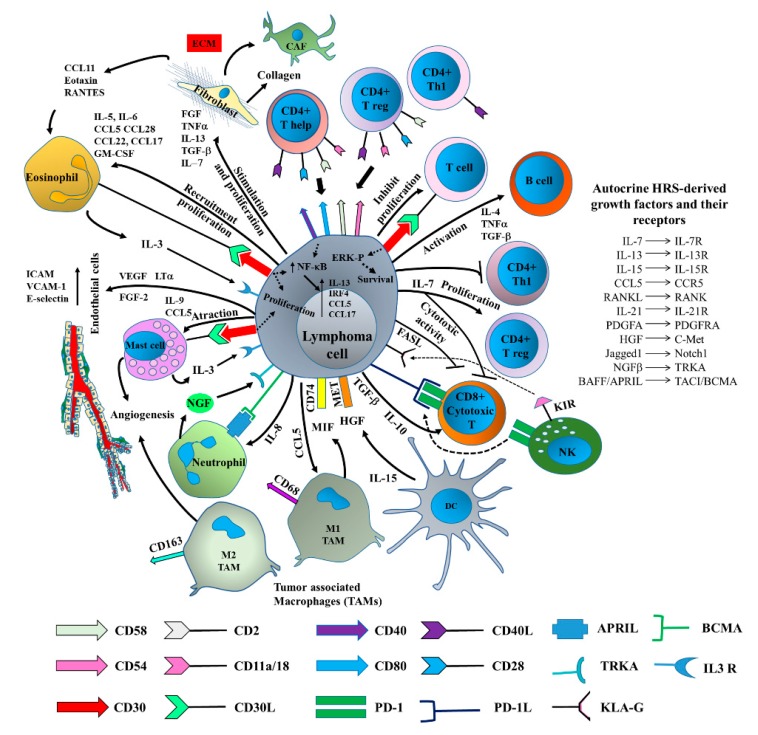
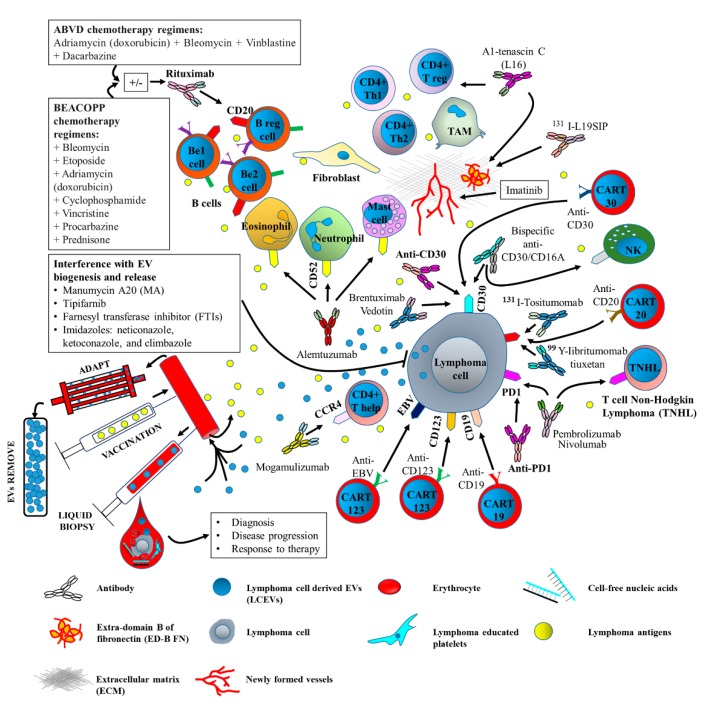
Lymphomas are heterogeneous diseases, and the term includes a number of histological subtypes that are characterized by different clinical behavior and molecular phenotypes. Valuable information on the presence of lymphoma cell-derived extracellular vesicles (LCEVs) in the bloodstream of patients suffering from this hematological cancer has recently been provided. In particular, it has been reported that the number and phenotype of LCEVs can both change as the disease progresses, as well as after treatment. Moreover, the role that LCEVs play in driving tumor immune escape has been reported. This makes LCEVs potential novel clinical tools for diagnosis, disease progression, and chemoresistance. LCEVs express surface markers and convey specific molecules in accordance with their cell of origin, which can be used as targets and thus lead to the development of specific therapeutics. This may be particularly relevant since circulating LCEVs are known to save lymphoma cells from anti-cluster of differentiation (CD)20-induced complement-dependent cytotoxicity. Therefore, effort should be directed toward investigating the feasibility of using LCEVs as predictive biomarkers of disease progression and/or response to treatment that can be translated to clinical use. The use of liquid biopsies in combination with serum EV quantification and cargo analysis have been also considered as potential approaches that can be pursued in the future. Upcoming research will also focus on the identification of specific molecular targets in order to generate vaccines and/or antibodies against LCEVs. Finally, the removal of circulating LCEVs has been proposed as a simple and non-invasive treatment approach. We herein provide an overview of the role of LCEVs in lymphoma diagnosis, immune tolerance, and drug resistance. In addition, alternative protocols that utilize LCEVs as therapeutic targets are discussed.
Keywords: extracellular vesicles; immunomodulation; innovative therapies; lymphoma.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures