

The diagnosis of multiple opportunistic infections in advanced stage AIDS: when Ockham's Razor doesn't cut it
- PMID: 30584503
- PMCID: PMC6287276
- DOI: 10.4322/acr.2018.028
The diagnosis of multiple opportunistic infections in advanced stage AIDS: when Ockham's Razor doesn't cut it
Abstract
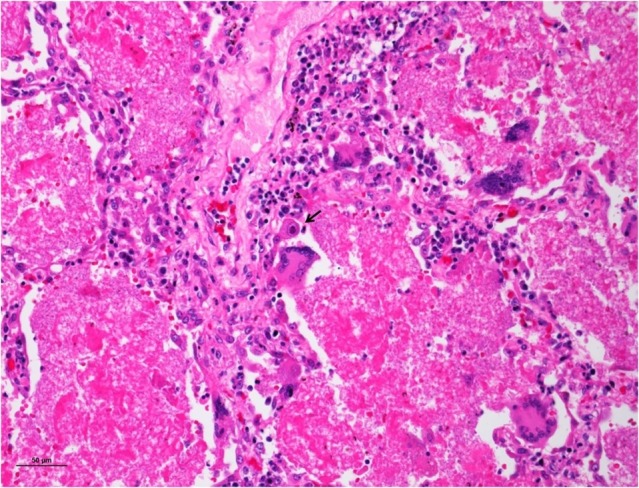
In the advanced stage of AIDS, the diagnosis of the opportunistic infections may be challenging due to the high risk of performing invasive diagnostic methods in a patient with a critical clinical condition, as well as the correct interpretation of the results of microbiological exams. One of the challenges for the diagnosis and treatment of the opportunistic infections is that they may occur concomitantly in the same patient and they may mimic each other, leading to a high discrepancy between clinical and autopsy diagnoses. We describe the case of a 52-year-old man who was hospitalized because of weight loss, anemia, cough, and hepatosplenomegaly. During the investigation, the diagnosis of AIDS was made, and the patient developed respiratory failure and died on the fourth day of hospitalization. At autopsy, disseminated non-tuberculosis mycobacteriosis was found, affecting mainly the organs of the reticuloendothelial system. Also, severe and diffuse pneumonia caused by multiple agents (Pneumocystis jirovecii , Histoplasma capsulatum, suppurative bacterial infection, non-tuberculosis mycobacteria, and cytomegalovirus) was seen in a morphological pattern that could be called "collision pneumonia." The lesson from this case, revealed by the autopsy, is that in advanced AIDS, patients often have multiple opportunistic infections, so the principle of Ockham's razor-that a single diagnosis is most likely the best diagnosis-fails in this clinical context.
Keywords: Acquired Immunodeficiency Syndrome; Cytomegalovirus; Histoplasma; Mycobacterium; Pneumocystis.
Conflict of interest statement
Conflict of interest: None
Figures











References
-
- Brasil . Ministério da Saúde . HIV/AIDS 2017 . Brasília: : Ministério da Saúde; ; 2017. . ( Boletim epidemiológico - Ano V nº 1- 27ª a 53ª semanas epidemiológicas - julho a dezembro de 2016, da 01ª a 26ª semanas epidemiológicas - janeiro a junho de 2017 ) [ cited 2017 Oct 12 ]. Available from: http://www.aids.gov.br/pt-br/pub/2017/boletim-epidemiologico-hivaids-201...
-
- Brasil . Ministério da Saúde . HIV/AIDS 2015 . Brasília: : Ministério da Saúde; ; 2015. . ( Boletim epidemiológico - HIV/AIDS. Ano IV nº 1 - 27ª à 53ª semana epidemiológica - julho a dezembro de 2014 da 01ª à 26ª semana epidemiológica - janeiro a junho de 2015 ). [ cited 2017 Jan 26 ]. Available from: http://www.aids.gov.br/sites/default/files/anexos/publicacao/2015/58534/...
-
- Coelho L , Veloso VG , Grinsztejn B , Luz PM . Trends in overall opportunistic illnesses, Pneumocystis carinii pneumonia, cerebral toxoplasmosis and Mycobacterium avium complex incidence rates over the 30 years of the HIV epidemic: a systematic review . Braz J Infect Dis . 2014. ; 18 ( 2 ): 196 - 210 . 10.1016/j.bjid.2013.10.003 . - DOI - PMC - PubMed
-
- Brasil . Ministério da Saúde . Perspectivas brasileiras para o fim da tuberculose como problema de saúde pública . Boletim Epidemiológico , 2016. ; 47 ( 13 ), 1 - 15 . [ cited 2017 Jan 26 ]. Available from http://portalsaude.saude.gov.br/images/pdf/2016/marco/24/2016-009-Tuberc...
