

Identifying Hesitation and Discomfort with Diagnosing Sepsis: Survey of a Pediatric Tertiary Care Center
- PMID: 30584626
- PMCID: PMC6221587
- DOI: 10.1097/pq9.0000000000000099
Identifying Hesitation and Discomfort with Diagnosing Sepsis: Survey of a Pediatric Tertiary Care Center
Abstract
Objective: Pediatric sepsis remains a significant cause of morbidity and mortality despite the development of strategies proven to improve diagnosis and treatment. Specifically, early recognition and urgent therapy initiation are consistently associated with improved outcomes. However, providers bring these principles inconsistently to the bedside. The objective of this study was to describe practitioner knowledge of, and attitudes toward, sepsis as a means of identifying potentially modifiable factors delaying life-saving treatment. We hypothesized there would be difficulties with sepsis recognition and self-reported discomfort with making the diagnosis among all provider groups in a pediatric tertiary care center.
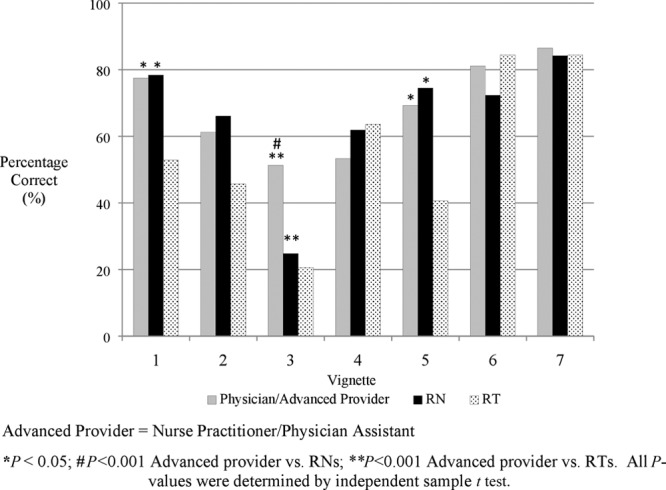
Methods: Emergency department and inpatient pediatric physicians, nurses, and respiratory therapists in a single, freestanding children's hospital received an electronic survey. Likert scales permitted anonymous self-reporting of comfort and diagnostic delays. Seven clinical vignettes assessed diagnostic knowledge. Independent sample t tests and Chi-square compared responses.
Results: Three hundred two staff participated (73% response rate), 41% of whom had at least 10 years of clinical experience. One in 5 was uncomfortable alerting coworkers to a patient with suspected sepsis or septic shock, and almost half were uncomfortable doing so in cases of compensated shock. Every role self-reported diagnostic delays, including faculty physicians. On average, physicians answered a greater percentage of vignette questions correctly (66%), compared with nurses (58%; P = 0.013) and respiratory therapists (52%; P = 0.005).
Conclusions: Sepsis knowledge deficits, provider discomfort, and diagnostic delays are prevalent within a tertiary care children's hospital. Their presence and scale suggest areas for future research and targeted intervention.
Figures
Similar articles
-
Impact of a Multidisciplinary Sepsis Initiative on Knowledge and Behavior in a Pediatric Center.Pediatr Qual Saf. 2020 Mar 10;5(2):e267. doi: 10.1097/pq9.0000000000000267. eCollection 2020 Mar-Apr. Pediatr Qual Saf. 2020. PMID: 32426633 Free PMC article.
-
Treatment of Pediatric Septic Shock With the Surviving Sepsis Campaign Guidelines and PICU Patient Outcomes.Pediatr Crit Care Med. 2016 Oct;17(10):e451-e458. doi: 10.1097/PCC.0000000000000906. Pediatr Crit Care Med. 2016. PMID: 27500722
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
-
Proadrenomedullin in Sepsis and Septic Shock: A Role in the Emergency Department.Medicina (Kaunas). 2021 Sep 1;57(9):920. doi: 10.3390/medicina57090920. Medicina (Kaunas). 2021. PMID: 34577843 Free PMC article. Review.
Cited by
-
Challenges and Solutions in translating sepsis guidelines into practice in resource-limited settings.Transl Pediatr. 2021 Oct;10(10):2646-2665. doi: 10.21037/tp-20-310. Transl Pediatr. 2021. PMID: 34765491 Free PMC article. Review.
-
Impact of a Multidisciplinary Sepsis Initiative on Knowledge and Behavior in a Pediatric Center.Pediatr Qual Saf. 2020 Mar 10;5(2):e267. doi: 10.1097/pq9.0000000000000267. eCollection 2020 Mar-Apr. Pediatr Qual Saf. 2020. PMID: 32426633 Free PMC article.
References
-
- Ruth A, McCracken CE, Fortenberry JD, et al. Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatr Crit Care Med. 2014;15:828–838.. - PubMed
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003;167:695–701.. - PubMed
-
- Watson RS, Carcillo JA. Scope and epidemiology of pediatric sepsis. Pediatr Crit Care Med. 2005;6:S3–S5.. - PubMed
-
- Weiss SL, Fitzgerald JC, Pappachan J, et al. ; Sepsis Prevalence, Outcomes, and Therapies (SPROUT) Study Investigators and Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network. Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study. Am J Respir Crit Care Med. 2015;191:1147–1157.. - PMC - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. ; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–1377.. - PubMed
LinkOut - more resources
Full Text Sources