

Response Heterogeneity With Exercise Training and Physical Activity Interventions Among Persons With Multiple Sclerosis
- PMID: 30585528
- PMCID: PMC6389390
- DOI: 10.1177/1545968318818904
Response Heterogeneity With Exercise Training and Physical Activity Interventions Among Persons With Multiple Sclerosis
Abstract
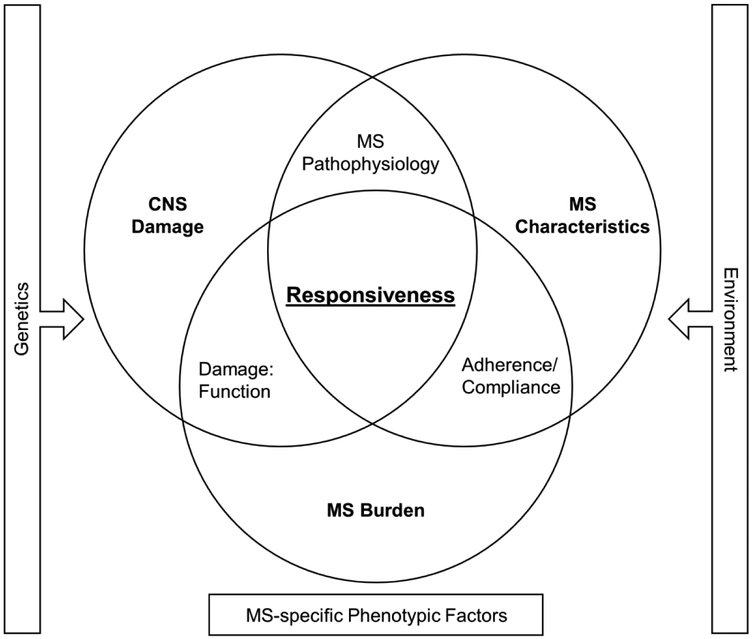
Multiple sclerosis (MS) is a heterogeneous disease, both in its pathology and symptomology. This poses a challenge for the medical management and rehabilitation of MS; however, physical activity and exercise training are rehabilitation approaches that have demonstrated beneficial effects on many of the burdensome consequences of MS such as mobility impairment and fatigue. Given the heterogeneous course of MS, it is possible that outcomes of physical activity and exercise training interventions demonstrate heterogeneity both in the magnitude and pattern of change, but there has been little focus on response heterogeneity with these interventions among persons with MS. In this narrative review, a search of the existing literature was performed to identify studies that reported individual participant data, which was used to describe the variability in the response to physical activity and exercise training interventions among persons with MS. Inter-individual variability seemingly occurs across outcomes and modalities, which underscores the consideration of factors that might influence response heterogeneity. Factors related to MS disease characteristics, nervous system damage, and the degree of MS-related disability might influence individual responsiveness. Large-scale studies that permit the examination of heterogeneity and its predictors will inform future research on the area of physical activity and exercise training in MS, and lead to the development of individually tailored rehabilitation approaches that will more effectively elicit change.
Keywords: exercise training; multiple sclerosis; physical activity; response heterogeneity.
Conflict of interest statement
Author Disclosures:
Competing Interests: None to disclose
Figures
Similar articles
-
Capitalising on the opinions of persons with multiple sclerosis to inform the main trial - participant opinions from participation in a feasibility study, a qualitative extension study.Disabil Rehabil. 2019 Dec;41(25):3071-3078. doi: 10.1080/09638288.2018.1490823. Epub 2018 Jul 24. Disabil Rehabil. 2019. PMID: 30039984
-
Response heterogeneity in fitness, mobility and cognition with exercise-training in MS.Acta Neurol Scand. 2019 Feb;139(2):183-191. doi: 10.1111/ane.13041. Epub 2018 Nov 19. Acta Neurol Scand. 2019. PMID: 30372515 Free PMC article.
-
Current perspectives on exercise training in the management of multiple sclerosis.Expert Rev Neurother. 2020 Aug;20(8):855-865. doi: 10.1080/14737175.2020.1796640. Epub 2020 Aug 1. Expert Rev Neurother. 2020. PMID: 32666855 Review.
-
Systematic Review on Exercise Training as a Neuroplasticity-Inducing Behavior in Multiple Sclerosis.Neurorehabil Neural Repair. 2020 Jul;34(7):575-588. doi: 10.1177/1545968320921836. Epub 2020 May 26. Neurorehabil Neural Repair. 2020. PMID: 32452269 Free PMC article.
-
Multimodal exercise training in multiple sclerosis: A randomized controlled trial in persons with substantial mobility disability.Contemp Clin Trials. 2017 Oct;61:39-47. doi: 10.1016/j.cct.2017.07.016. Epub 2017 Jul 19. Contemp Clin Trials. 2017. PMID: 28732757 Clinical Trial.
Cited by
-
Heterogeneity of aerobic fitness changes with exercise training in progressive multiple sclerosis: Secondary, exploratory analysis of data from the CogEx trial.Mult Scler J Exp Transl Clin. 2024 Dec 5;10(4):20552173241301030. doi: 10.1177/20552173241301030. eCollection 2024 Oct-Dec. Mult Scler J Exp Transl Clin. 2024. PMID: 39651332 Free PMC article.
-
Randomized Controlled Trial of the Behavioral Intervention for Physical Activity in Multiple Sclerosis Project: Response Heterogeneity and Predictors of Change.Int J Behav Med. 2025 Feb;32(1):69-79. doi: 10.1007/s12529-024-10265-7. Epub 2024 Feb 7. Int J Behav Med. 2025. PMID: 38326673 Clinical Trial.
-
Predictors of positive outcomes following resistive inspiratory muscle training in non-ambulatory persons with advanced multiple sclerosis.Mult Scler J Exp Transl Clin. 2022 May 23;8(2):20552173211058862. doi: 10.1177/20552173211058862. eCollection 2022 Apr-Jun. Mult Scler J Exp Transl Clin. 2022. PMID: 35634011 Free PMC article.
-
The meaningfulness of exploring one's own limits through interactions and enjoyment in outdoor high-intensity physiotherapy for people with multiple sclerosis: a qualitative study.Front Rehabil Sci. 2024 Mar 18;5:1303094. doi: 10.3389/fresc.2024.1303094. eCollection 2024. Front Rehabil Sci. 2024. PMID: 38566621 Free PMC article.
-
Cardiopulmonary Exercise Testing Using the Modified Balke Protocol in Fully Ambulatory People With Multiple Sclerosis.Cardiopulm Phys Ther J. 2021 Apr;32(2):57-65. doi: 10.1097/cpt.0000000000000141. Epub 2020 Oct 15. Cardiopulm Phys Ther J. 2021. PMID: 36380901 Free PMC article.
References
-
- Siffrin V, Vogt J, Radbruch H, Nitsch R, Zipp F. Multiple sclerosis–candidate mechanisms underlying CNS atrophy. Trends in neurosciences. 2010;33(4):202–210. - PubMed
-
- Pearson M, Dieberg G, Smart N. Exercise as a therapy for improvement of walking ability in adults with multiple sclerosis: a meta-analysis. Archives of physical medicine and rehabilitation. 2015;96(7):1339–1348. e1337. - PubMed
-
- Snook EM, Motl RW. Effect of exercise training on walking mobility in multiple sclerosis: a meta-analysis. Neurorehabilitation and neural repair. 2009;23(2):108–116. - PubMed
-
- Learmonth YC, Ensari I, Motl RW. Physiotherapy and walking outcomes in adults with multiple sclerosis: systematic review and meta-analysis. Physical Therapy Reviews. 2016;21(3–6):160–172.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
