

Empagliflozin in posttransplantation diabetes mellitus: A prospective, interventional pilot study on glucose metabolism, fluid volume, and patient safety
- PMID: 30585690
- PMCID: PMC6590167
- DOI: 10.1111/ajt.15223
Empagliflozin in posttransplantation diabetes mellitus: A prospective, interventional pilot study on glucose metabolism, fluid volume, and patient safety
Abstract
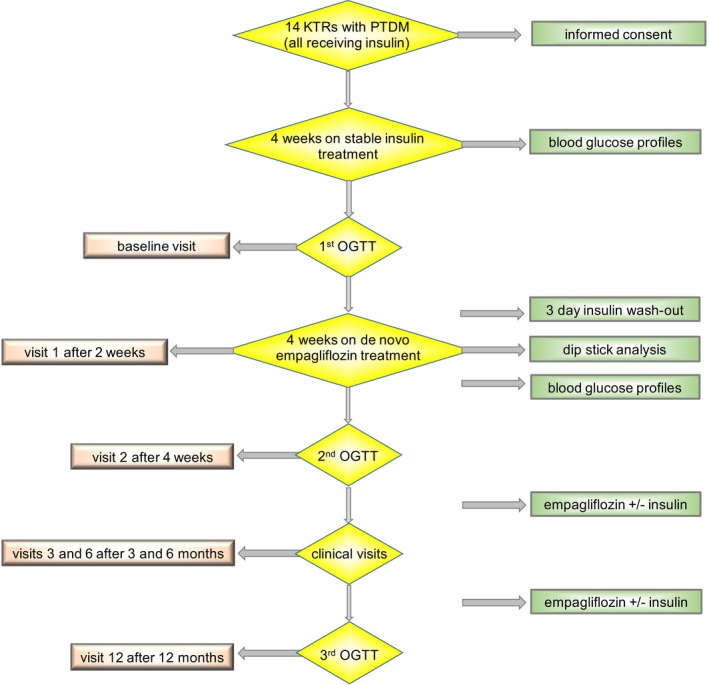
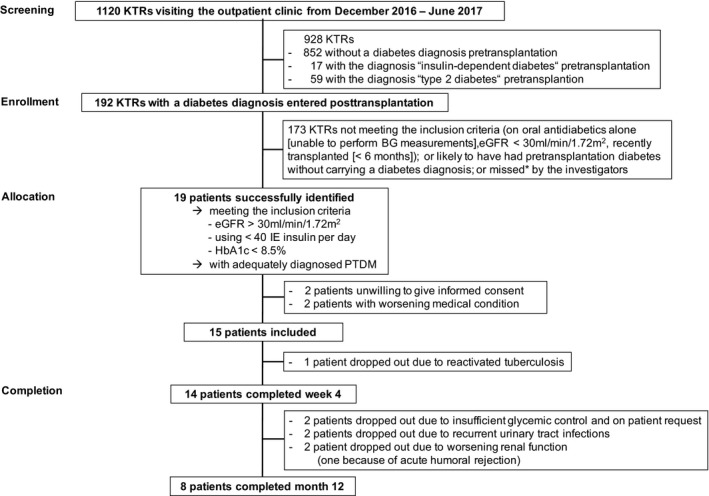
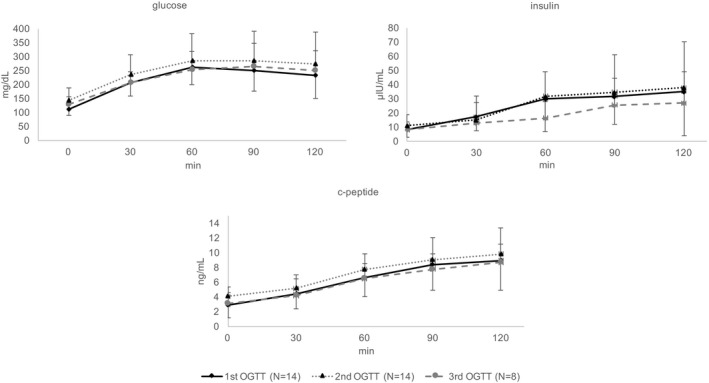
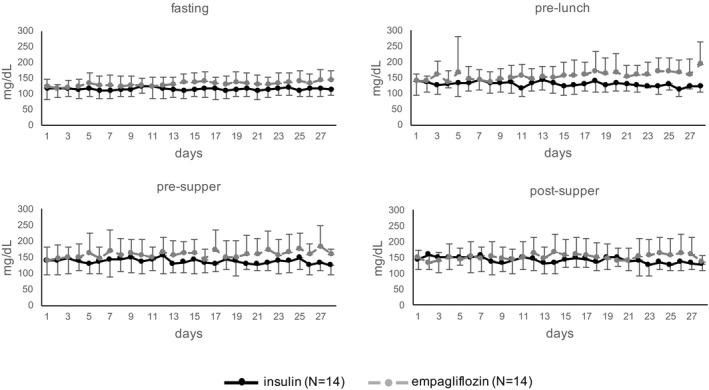
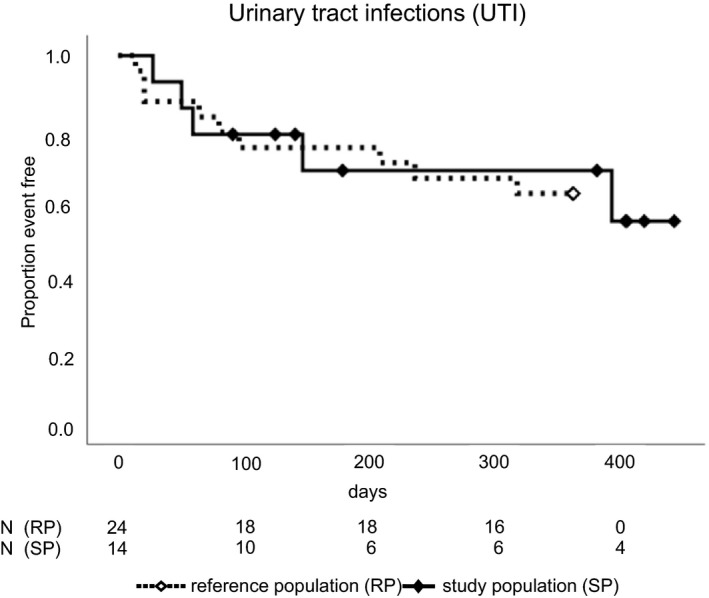
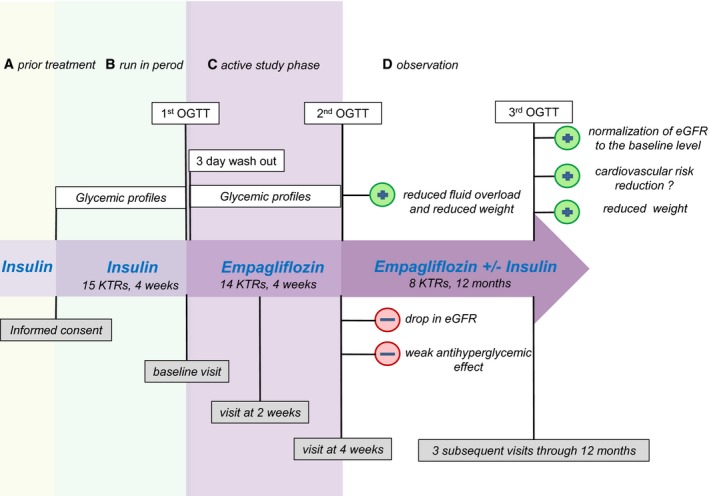
The safety and efficacy of sodium-glucose cotransporter 2 inhibitors in posttransplantation diabetes mellitus is unknown. We converted stable kidney transplant patients to 10 mg empagliflozin, aiming at replacing their insulin therapy (<40 IU/d). N = 14 participants (the required sample size) completed the study visits through 4 weeks and N = 8 through 12 months. Oral glucose tolerance test (OGTT)-derived 2-hour glucose (primary end point) increased from 232 ± 82 mg/dL (baseline) to 273 ± 116 mg/dL (4 weeks, P = .06) and to 251 ± 71 mg/dL (12 months, P = .41). Self-monitored blood glucose and hemoglobin A1c were also clinically inferior with empagliflozin monotherapy, such that insulin was reinstituted in 3 of 8 remaining participants. Five participants (2 of them dropouts) vs nine of 24 matched reference patients developed bacterial urinary tract infections (P = .81). In empagliflozin-treated participants, oral glucose insulin sensitivity decreased and beta-cell glucose sensitivity increased at the 4-week and 12-month OGTTs. Estimated glomerular filtration rate and bioimpedance spectroscopy-derived extracellular and total body fluid volumes decreased by 4 weeks, but recovered. All participants lost body weight. No participant developed ketoacidosis; 1 patient developed balanitis. In conclusion, although limited by sample size and therefore preliminary, these results suggest that empagliflozin can safely be used as add-on therapy, if posttransplant diabetes patients are monitored closely (NCT03113110).
Keywords: clinical research/practice; diabetes: new onset/posttransplant; endocrinology/diabetology; kidney (allograft) function/dysfunction; kidney transplantation/nephrology; metabolism/metabolite.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Sharif A, Baboolal K. Complications associated with new‐onset diabetes after kidney transplantation. Nat Rev Nephrol. 2011;8(1):34‐42. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
