

Use of Computerized Provider Order Entry Events for Postoperative Complication Surveillance
- PMID: 30586132
- PMCID: PMC6484794
- DOI: 10.1001/jamasurg.2018.4874
Use of Computerized Provider Order Entry Events for Postoperative Complication Surveillance
Abstract
Importance: Conventional approaches for tracking postoperative adverse events requires manual medical record review, thus limiting the scalability of such efforts.
Objective: To determine if a surveillance system using computerized provider order entry (CPOE) events for selected medications as well as laboratory, microbiologic, and radiologic orders can decrease the manual medical record review burden for surveillance of postoperative complications.
Design, setting, and participants: This cohort study reviewed the medical records of 21 775 patients who underwent surgical procedures at a university-based tertiary referral center (University of Utah, Salt Lake City) from July 1, 2007, to August 31, 2017. Patients were included if their case was selected for review by a surgical clinical reviewer as part of the National Surgical Quality Improvement Program. Patients were excluded if they had incomplete follow-up data.
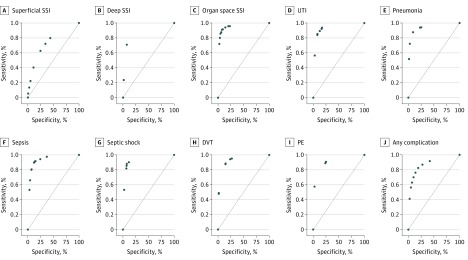
Main outcomes and measures: Thirty-day postoperative occurrences of superficial surgical site infection, deep surgical site infection, organ space surgical site infection, urinary tract infection, pneumonia, sepsis, septic shock, deep vein thrombosis requiring therapy, and pulmonary embolism, as defined by the National Surgical Quality Improvement Program. A logistic regression model was developed for each postoperative complication using CPOE features as predictors on a development set, and performance was measured on a holdout internal validation set. The models were internally validated using bootstrapping with 10 000 replications to determine the sensitivity, specificity, positive predictive value, and negative predictive value of CPOE-based surveillance system.
Results: The study included 21 775 patients who underwent surgical procedures. Among these patients, 11 855 (54.4%) were women and 9920 (45.6%) were men, with a mean (SD) age of 51.7 (16.8) years. Overall, the prevalence of postoperative complications was low, ranging from 0.2% (pulmonary embolism) to 2.6% (superficial surgical site infection). Use of CPOE events to detect patients who experienced at least 1 complication had a sensitivity of 74.8% (95% CI, 71.1%-78.4%), specificity of 86.8% (95% CI, 85.5%-88.3%), positive predictive value of 33.8% (95% CI, 31.2%-36.4%), negative predictive value of 97.5% (95% CI, 97.1%-97.8%), and area under the curve of 0.808 (95% CI, 0.791-0.824). The negative predictive value for individual complications ranged from 98.7% to 100%. Use of CPOE events to screen for adverse events was estimated to diminish the burden of manual medical record review by 55.4% to 90.3%. A CPOE-based surveillance system performed well for both inpatient and outpatient procedures.
Conclusions and relevance: A CPOE-based surveillance of postoperative complications has high negative predictive value, which demonstrates that this approach can augment the currently used, resource-intensive manual medical record review process.
Conflict of interest statement
Figures
References
-
- Hall BL, Hamilton BH, Richards K, Bilimoria KY, Cohen ME, Ko CY. Does surgical quality improve in the American College of Surgeons National Surgical Quality Improvement Program: an evaluation of all participating hospitals. Ann Surg. 2009;250(3):363-376. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
