

Associations between birth kit use and maternal and neonatal health outcomes in rural Jigawa state, Nigeria: A secondary analysis of data from a cluster randomized controlled trial
- PMID: 30586441
- PMCID: PMC6306201
- DOI: 10.1371/journal.pone.0208885
Associations between birth kit use and maternal and neonatal health outcomes in rural Jigawa state, Nigeria: A secondary analysis of data from a cluster randomized controlled trial
Abstract
Background: The burden of maternal and neonatal mortality remains persistently high in Nigeria. Sepsis contributes significantly to both maternal and newborn mortality, and safe delivery kits have long been promoted as a cost-effective intervention to ensure hygienic delivery practices and reduce sepsis. However, there is limited evidence on the effectiveness of home birth kit distribution by community health workers, and particularly the impact of this intervention on health outcomes. This paper reports a secondary analysis of data from a cluster randomized trial in rural northern Nigeria in which birth kits were distributed by community health workers to pregnant women in their homes, analyzing non-experimental variation in receipt and use of birth kits. More specifically, associations between pregnant women's baseline characteristics and receipt and use of birth kits, and associations between birth kit use, care utilization and maternal and newborn outcomes were assessed.
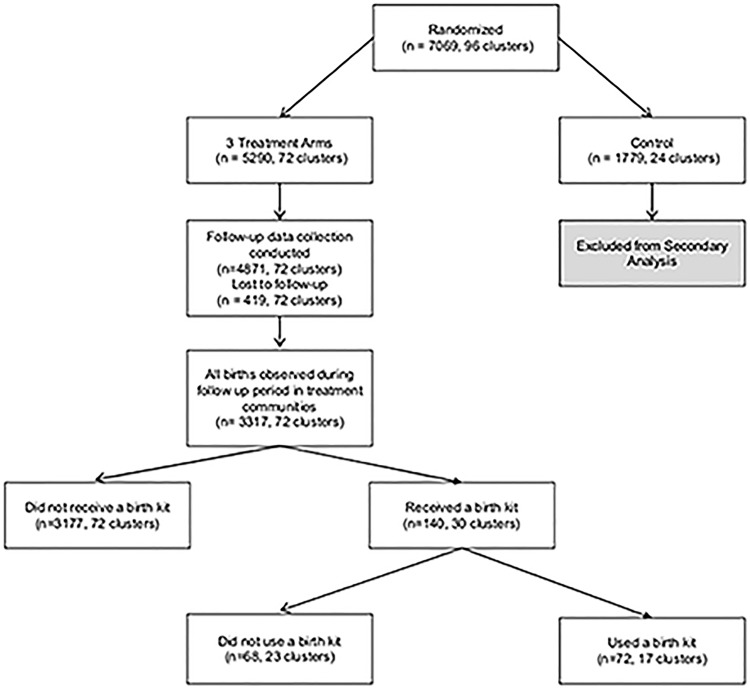
Methods and findings: Baseline, post-birth and endline data related to 3,317 births observed over a period of three years in 72 intervention communities in Jigawa state, Nigeria, were analyzed using hierarchical, logistic regression models. In total, 140 women received birth kits, and 72 women used the kits. There were no associations between baseline demographic characteristics, health history, and knowledge and attitudes and receipt of a kit, suggesting that community health workers did not systematically target the distribution of birth kits. However, women who used the kit reported reduced odds of past pregnancy complications (OR = 0.44, 95% CI: 0.19-1.00) as well as significantly higher odds of feeling generally healthy at baseline (OR = 2.00, 95% CI: 1.06-3.76), of exposure to radio media (OR = 1.97, 95% CI: 1.21-3.22), and of perceiving themselves as having a low-risk pregnancy (OR = 3.05, 95% CI:1.39-6.68). While there were no significant associations between birth kit use and facility based delivery, skilled birth attendance or post-natal care, women who used a kit exhibited significantly lower odds of completing four or more ANC visits (adjusted OR = 0.39, 95% CI: 0.18-0.85) and significantly higher odds of reporting prolonged labor (adjusted OR = 4.75, 95% CI: 1.36-16.59), and post-partum bleeding (adjusted OR = 3.25, 95% CI: 1.11-9.52).
Conclusions: This evidence suggests that use of birth kits is low in a rural population characterized by minimal baseline utilization of maternal and neonatal health services, and the use of birth kits was not associated with reductions in maternal or neonatal morbidity. While further research is required to understand how the effectiveness of birth kits may be shaped by the mechanism through which women access and utilize the kits, our findings suggest that the provision of kits to women outside of the formal health system may be associated with increased risk of adverse outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Evaluation of a community-based intervention package to improve knowledge of obstetric danger signs, birth preparedness, and institutional delivery care utilization in Arba Minch Zuria District, Ethiopia: a cluster-randomized trial.Reprod Health. 2023 Nov 18;20(1):169. doi: 10.1186/s12978-023-01713-w. Reprod Health. 2023. PMID: 37980484 Free PMC article. Clinical Trial.
-
Effects of women's groups practising participatory learning and action on preventive and care-seeking behaviours to reduce neonatal mortality: A meta-analysis of cluster-randomised trials.PLoS Med. 2017 Dec 5;14(12):e1002467. doi: 10.1371/journal.pmed.1002467. eCollection 2017 Dec. PLoS Med. 2017. PMID: 29206833 Free PMC article.
-
"That's a woman's problem": a qualitative analysis to understand male involvement in maternal and newborn health in Jigawa state, northern Nigeria.Reprod Health. 2019 Sep 18;16(1):143. doi: 10.1186/s12978-019-0808-4. Reprod Health. 2019. PMID: 31533839 Free PMC article.
-
Community-based maternal and newborn educational care packages for improving neonatal health and survival in low- and middle-income countries.Cochrane Database Syst Rev. 2019 Nov 5;2019(11):CD007647. doi: 10.1002/14651858.CD007647.pub2. Cochrane Database Syst Rev. 2019. PMID: 31686427 Free PMC article.
-
Systematic review of community participation interventions to improve maternal health outcomes in rural South Asia.BMC Pregnancy Childbirth. 2018 Aug 10;18(1):327. doi: 10.1186/s12884-018-1964-1. BMC Pregnancy Childbirth. 2018. PMID: 30097022 Free PMC article.
Cited by
-
Can Clean Delivery Kits Prevent Infections? Lessons from Traditional Birth Attendants in Nigeria.Ann Glob Health. 2023 Dec 6;89(1):85. doi: 10.5334/aogh.4015. eCollection 2023. Ann Glob Health. 2023. PMID: 38077261 Free PMC article. Clinical Trial.
-
Genome-wide association study reveals marker-trait associations for major agronomic traits in proso millet (Panicum miliaceum L.).Planta. 2024 Jul 4;260(2):44. doi: 10.1007/s00425-024-04465-4. Planta. 2024. PMID: 38963439
-
Types, reporting and acceptability of community-based interventions for stillbirth prevention in sub-Saharan Africa (SSA): a systematic review.EClinicalMedicine. 2023 Aug 3;62:102133. doi: 10.1016/j.eclinm.2023.102133. eCollection 2023 Aug. EClinicalMedicine. 2023. PMID: 37593225 Free PMC article.
-
Safe delivery kits and newborn infection in rural Ethiopian communities.Front Public Health. 2024 Aug 9;12:1305255. doi: 10.3389/fpubh.2024.1305255. eCollection 2024. Front Public Health. 2024. PMID: 39185109 Free PMC article.
-
The complexity of kodo millet: genomic analysis and implications in crop improvement.Planta. 2024 Dec 16;261(1):15. doi: 10.1007/s00425-024-04588-8. Planta. 2024. PMID: 39680216 Review.
References
-
- NPC and ICF International. Nigeria Demographic and Health Survey; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
