

Non-inferior low-dose coronary computed tomography angiography image quality with knowledge-based iterative model reconstruction for overweight patients
- PMID: 30586449
- PMCID: PMC6306215
- DOI: 10.1371/journal.pone.0209243
Non-inferior low-dose coronary computed tomography angiography image quality with knowledge-based iterative model reconstruction for overweight patients
Abstract
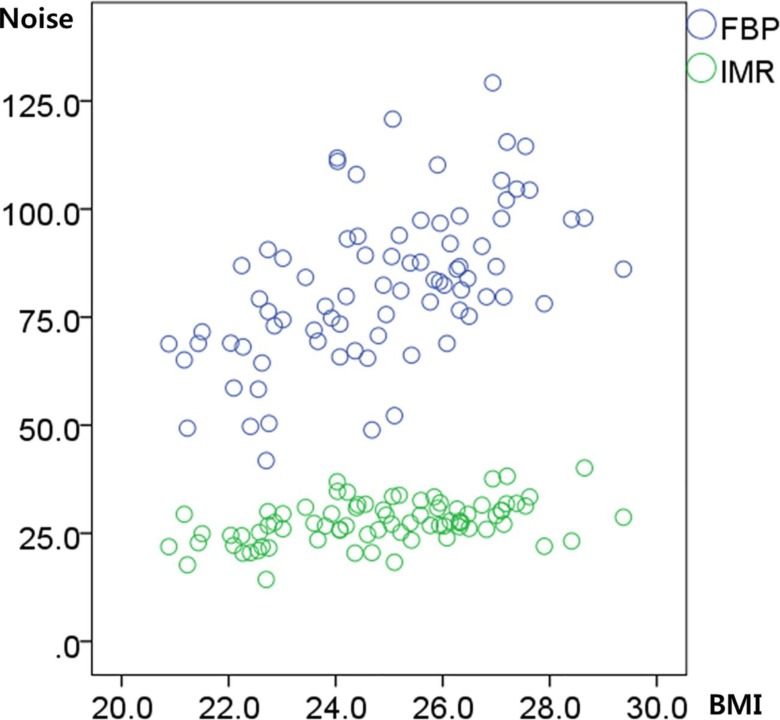
We investigated the feasibility of low-dose coronary computed tomography angiography (CCTA), using a prospective electrocardiogram (ECG)-triggered axial scan protocol, knowledge-based iterative model reconstruction (IMR), and fixed tube current, in overweight subjects. Forty non-overweight (group A; body-mass index [BMI] < 25 kg/m2) and 40 overweight individuals (group B; BMI = 25-30 kg/m2), who underwent CCTA for coronary artery disease screening, were retrospectively and consecutively enrolled. A 64-slice CT scanner was used at 100-kVp tube voltage and 150-mA tube current, and images were reconstructed using IMR techniques. Image noise, attenuation at the aorta, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR) at the proximal right and left main coronary arteries (pRCA and LMCA) were calculated. CCTA images were qualitatively evaluated using a four-point scale (1, poor; 4, excellent) and analyzed using a non-inferiority test with a pre-defined non-inferiority margin of -0.2. The mean CCTA radiation dose (Group A: 1.33 ± 0.02 mSv; Group B: 1.35 ± 0.10 mSv; p = 0.151) and mean aortic root CT attenuation values (Group A: 447.9 ± 81.6 HU; Group B: 439.5 ± 63.6 HU; p = 0.571) did not differ significantly between the two groups. The mean noise in groups A and B was 26.0 ± 4.8 HU and 29.2 ± 4.4 HU, respectively (p = 0.005). The noise reduction ratio in the groups, compared to filtered back projection, was 65.0% and 68.1%, respectively. The mean grade of image quality did not differ significantly (3.75 ± 0.04 vs. 3.71 ± 0.04, p = 0.478). Group B CCTA image quality was non-inferior (mean difference = -0.043, 95% CI = -0.162-0.077) to that of Group A. We concluded that low-dose CCTA with prospective ECG-triggering and IMR might be applied to overweight subjects, as well as to normal-weight subjects, by using a fixed tube current without an increase in tube current based on the patient's body size.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hausleiter J, Martinoff S, Hadamitzky M, Martuscelli E, Pschierer I, Feuchtner GM, et al. Image quality and radiation exposure with a low tube voltage protocol for coronary CT angiography results of the PROTECTION II Trial. JACC Cardiovasc Imaging. 2010;3: 1113–1123. 10.1016/j.jcmg.2010.08.016 - DOI - PubMed
-
- Hausleiter J, Meyer TS, Martuscelli E, Spagnolo P, Yamamoto H, Carrascosa P, et al. Image quality and radiation exposure with prospectively ECG-triggered axial scanning for coronary CT angiography: the multicenter, multivendor, randomized PROTECTION-III study. JACC Cardiovasc Imaging. 2012;5: 484–493. 10.1016/j.jcmg.2011.12.017 - DOI - PubMed
-
- Deseive S, Pugliese F, Meave A, Alexanderson E, Martinoff S, Hadamitzky M, et al. Image quality and radiation dose of a prospectively electrocardiography-triggered high-pitch data acquisition strategy for coronary CT angiography: The multicenter, randomized PROTECTION IV study. J Cardiovasc Comput Tomogr. 2015;9: 278–285. 10.1016/j.jcct.2015.03.001 - DOI - PubMed
-
- Deseive S, Chen MY, Korosoglou G, Leipsic J, Martuscelli E, Carrascosa P, et al. Prospective randomized trial on radiation dose estimates of CT angiography applying iterative image reconstruction: the PROTECTION V study. JACC Cardiovasc Imaging. 2015;8: 888–896. 10.1016/j.jcmg.2015.02.024 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
