

Relationship Between Operator Volume and Long-Term Outcomes After Percutaneous Coronary Intervention
- PMID: 30586696
- PMCID: PMC6340715
- DOI: 10.1161/CIRCULATIONAHA.117.033325
Relationship Between Operator Volume and Long-Term Outcomes After Percutaneous Coronary Intervention
Abstract
Background: Although many studies show an inverse association between operator procedural volume and short-term adverse outcomes after percutaneous coronary intervention (PCI), the association between procedural volume and longer-term outcomes is unknown.
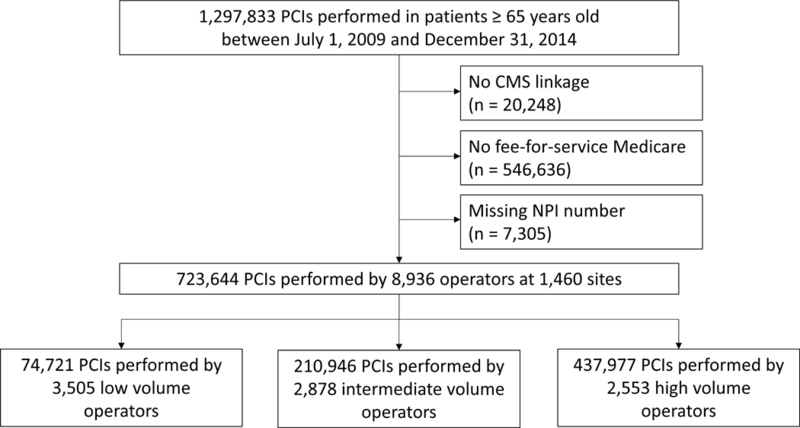
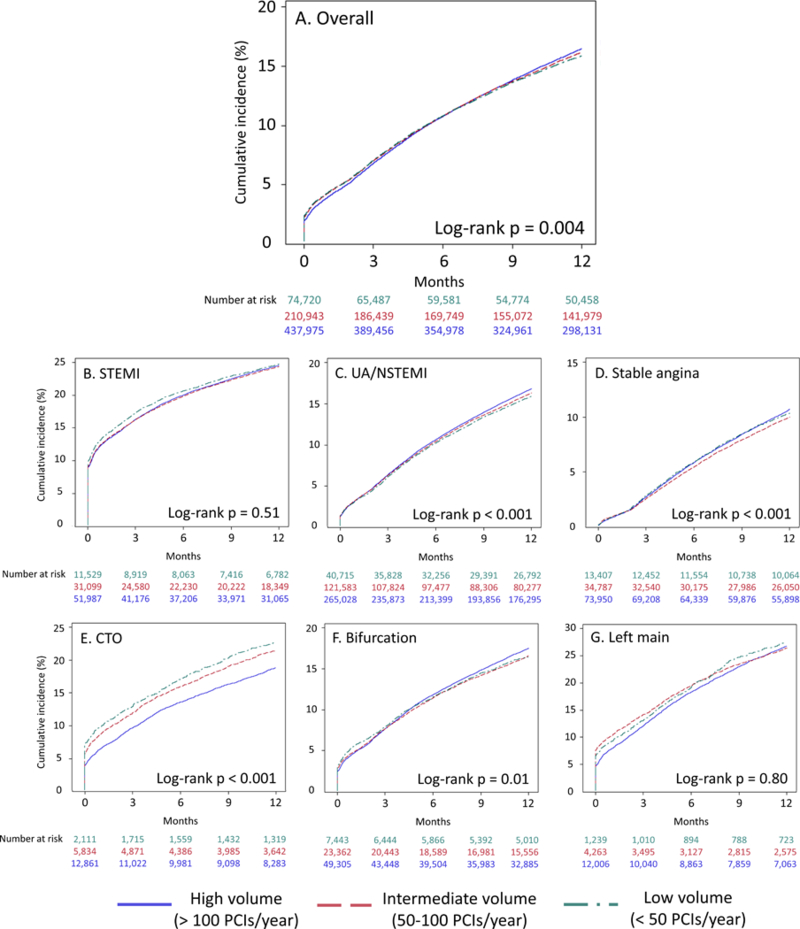
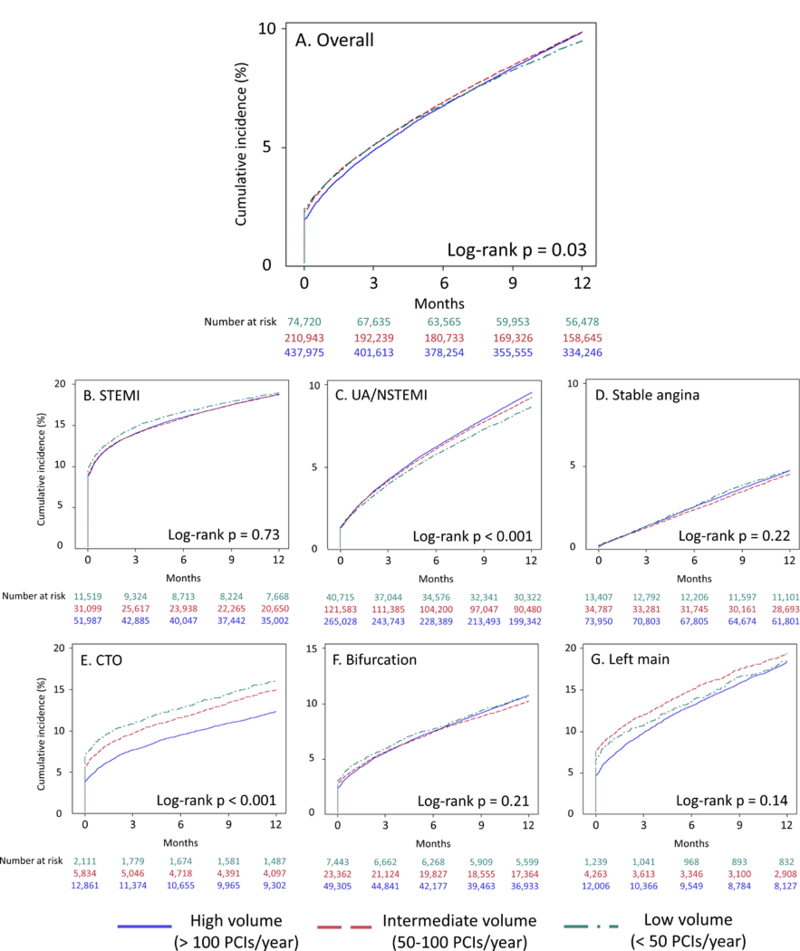
Methods: Using the National Cardiovascular Data Registry CathPCI registry data linked with Medicare claims data, we examined the association between operator PCI volume and long-term outcomes among patients ≥65 years of age. Operators were stratified by average annual PCI volume (counting PCIs performed in patients of all ages): low- (<50 PCIs), intermediate- (50-100), and high- (>100) volume operators. One-year unadjusted rates of death and major adverse coronary events (MACEs; defined as death, readmission for myocardial infarction, or unplanned coronary revascularization) were calculated with Kaplan-Meier methods. The proportional hazards assumption was not met, and risk-adjusted associations between operator volume and outcomes were calculated separately from the time of PCI to hospital discharge and from hospital discharge to 1-year follow-up.
Results: Between July 1, 2009, and December 31, 2014, 723 644 PCI procedures were performed by 8936 operators: 2553 high-, 2878 intermediate-, and 3505 low-volume operators. Compared with high- and intermediate-volume operators, low-volume operators more often performed emergency PCI, and their patients had fewer cardiovascular comorbidities. Over 1-year follow-up, 15.9% of patients treated by low-volume operators had a MACE compared with 16.9% of patients treated by high-volume operators ( P=0.004). After multivariable adjustment, intermediate- and high-volume operators had a significantly lower rate of in-hospital death than low-volume operators (odds ratio, 0.91; 95% CI, 0.86-0.96 for intermediate versus low; odds ratio, 0.79; 95% CI, 0.75-0.83 for high versus low). There were no significant differences in rates of MACEs, death, myocardial infarction, or unplanned revascularization between operator cohorts from hospital discharge to 1-year follow-up (adjusted hazard ratio for MACEs, 0.99; 95% CI, 0.96-1.01 for intermediate versus low; hazard ratio, 1.01; 95% CI, 0.99-1.04 for high versus low).
Conclusions: Unadjusted 1-year outcomes after PCI were worse for older adults treated by operators with higher annual volume; however, patients treated by these operators had more cardiovascular comorbidities. After risk adjustment, higher operator volume was associated with lower in-hospital mortality and no difference in postdischarge MACEs.
Keywords: morbidity; mortality; outcome assessment (health care); percutaneous coronary intervention; stents.
Figures
Comment in
-
A New Dimension in the Relationship Between Procedural Volumes and Quality.Circulation. 2019 Jan 22;139(4):473-476. doi: 10.1161/CIRCULATIONAHA.118.037383. Circulation. 2019. PMID: 30664378 No abstract available.
References
-
- Hannan EL, Racz M, Ryan TJ, McCallister BD, Johnson LW, Arani DT, Guerci AD, Sosa J and Topol EJ. Coronary angioplasty volume-outcome relationships for hospitals and cardiologists. J Am Med Assoc. 1997;277:892–898. - PubMed
-
- McGrath PD, Wennberg DE, Malenka DJ, Kellett MA, Ryan TJ, O’Meara JR, Bradley WA, Hearne MJ, Hettleman B and Robb JF. Operator volume and outcomes in 12,988 percutaneous coronary interventions. J Am Coll Cardiol. 1998;31:570–576. - PubMed
-
- Moscucci M, Share D, Smith D, O’Donnell MJ, Riba A, McNamara R, Lalonde T, Defranco AC, Patel K and Rogers EK. Relationship between operator volume and adverse outcome in contemporary percutaneous coronary intervention practice: an analysis of a quality-controlled multicenter percutaneous coronary intervention clinical database. J Am Coll Cardiol. 2005;46:625–632. - PubMed
-
- Minges KE, Wang Y, Dodson JA, Normand S-LT, Rathore SS, Ting HH, Nallamothu BK, Messenger J, Krumholz HM and Curtis JP. Physician Annual Volume and In-Hospital Mortality Following Percutaneous Coronary Intervention. Circulation. 2011;124:A16550.
-
- Badheka AO, Patel NJ, Grover P, Singh V, Patel N, Arora S, Chothani A, Mehta K, Deshmukh A and Savani GT. Impact of annual operator and institutional volume on percutaneous coronary intervention outcomes: a 5-year United States experience (2005–2009). Circulation. 2014;130:1392–1406. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
