

Genetically Determined Levels of Circulating Cytokines and Risk of Stroke
- PMID: 30586705
- PMCID: PMC7477819
- DOI: 10.1161/CIRCULATIONAHA.118.035905
Genetically Determined Levels of Circulating Cytokines and Risk of Stroke
Abstract
Background: Cytokines and growth factors have been implicated in the initiation and propagation of vascular disease. Observational studies have shown associations of their circulating levels with stroke. Our objective was to explore whether genetically determined circulating levels of cytokines and growth factors are associated with stroke and its etiologic subtypes by conducting a 2-sample Mendelian randomization (MR) study.
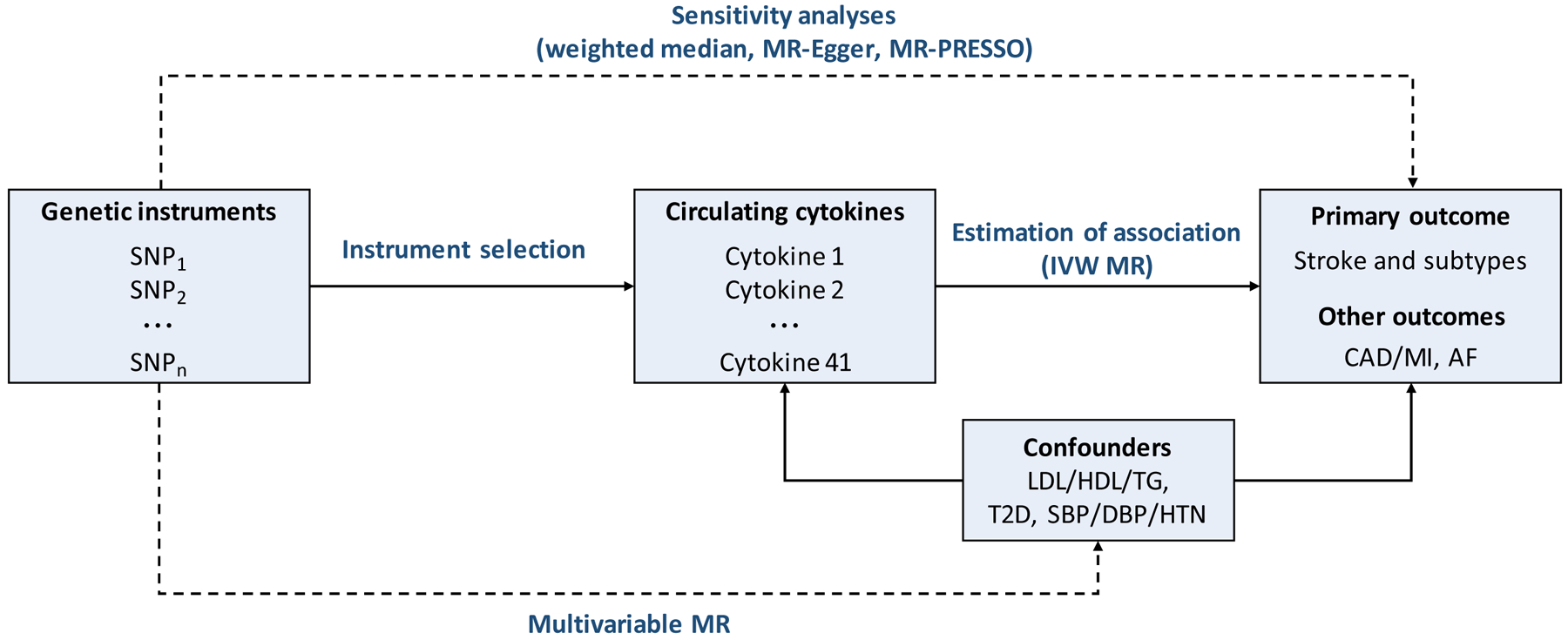
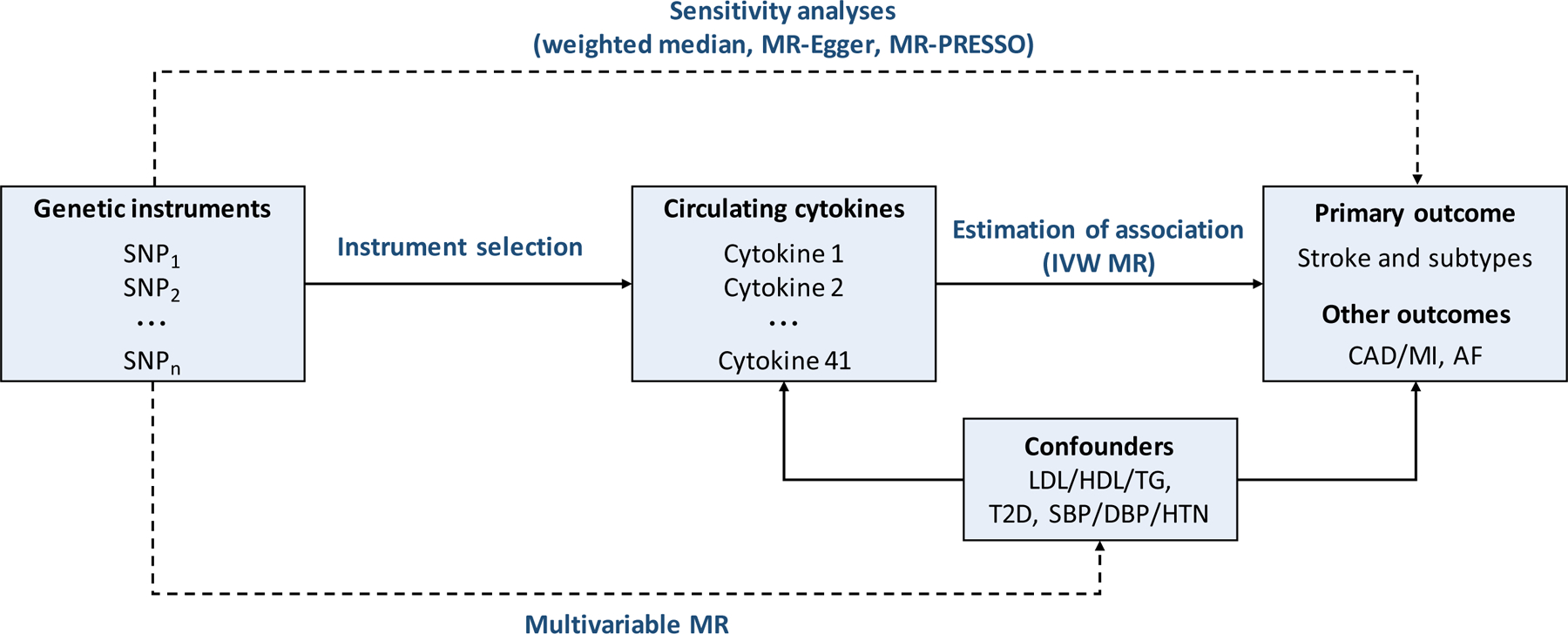
Methods: Genetic instruments for 41 cytokines and growth factors were obtained from a genome-wide association study of 8293 healthy adults. Their associations with stroke and stroke subtypes were evaluated in the MEGASTROKE genome-wide association study data set (67 162 cases; 454 450 controls) applying inverse variance-weighted meta-analysis, weighted-median analysis, Mendelian randomization-Egger regression, and multivariable Mendelian randomization. The UK Biobank cohort was used as an independent validation sample (4985 cases; 364 434 controls). Genetic instruments for monocyte chemoattractant protein-1 (MCP-1/CCL2) were further tested for association with etiologically related vascular traits by using publicly available genome-wide association study data.
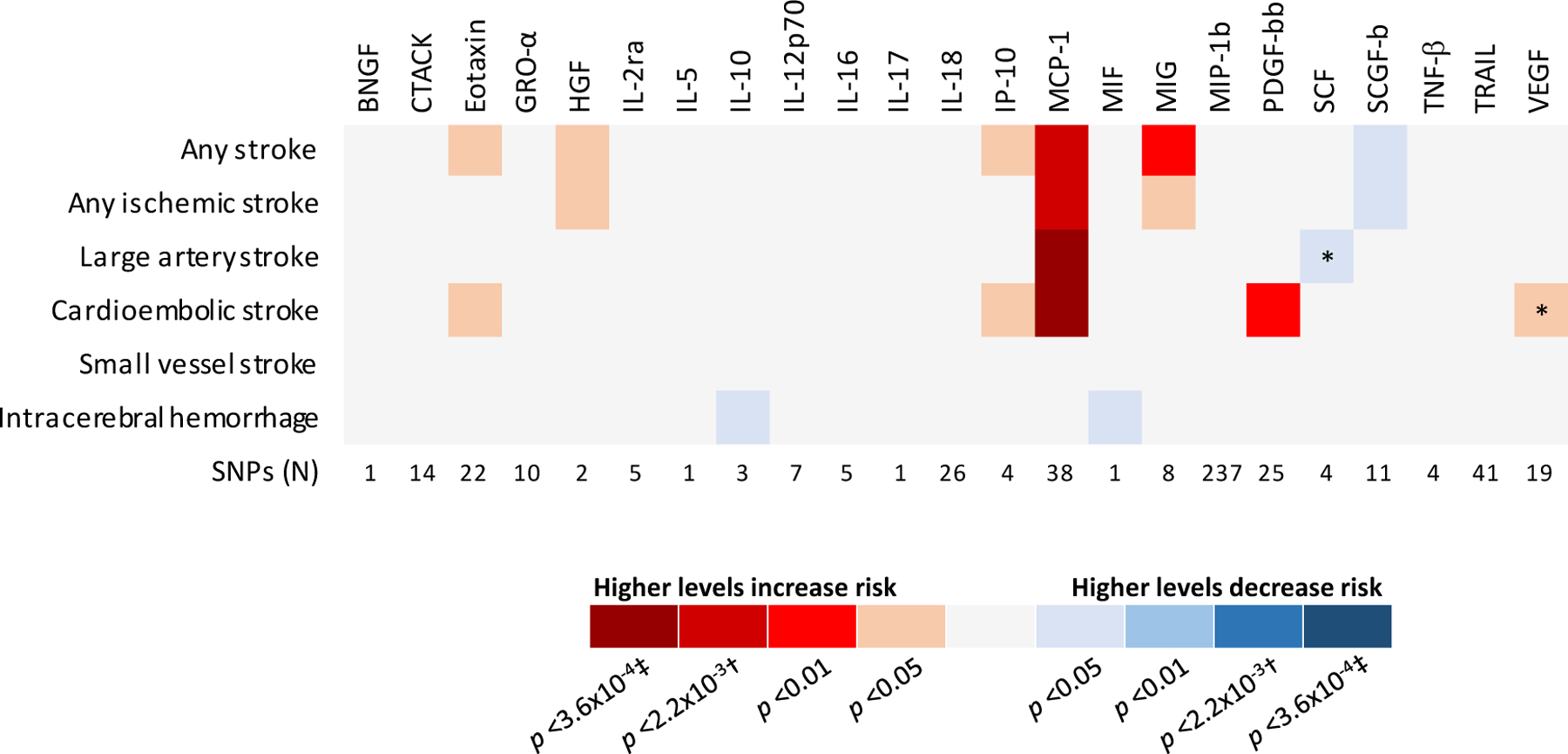
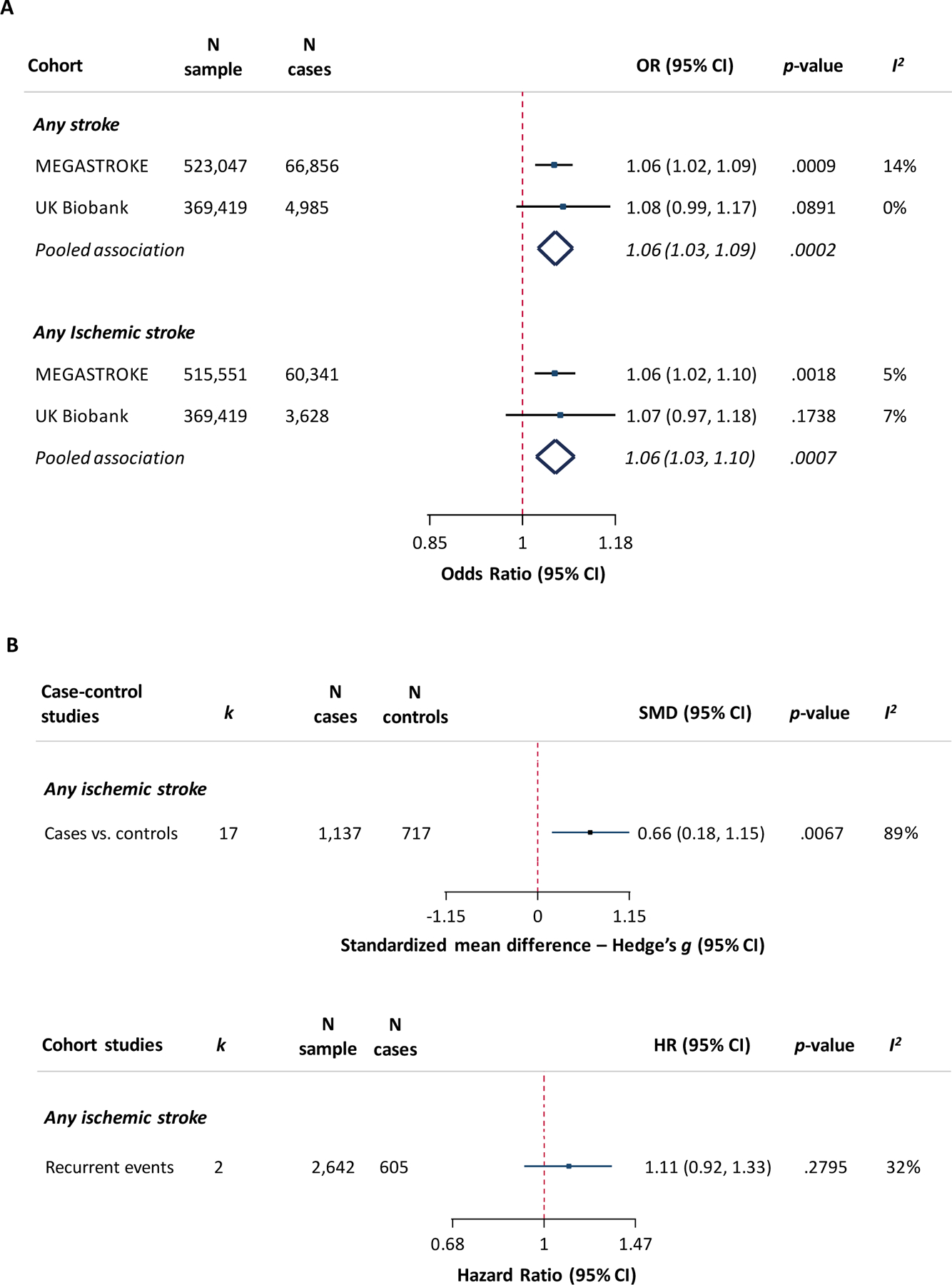
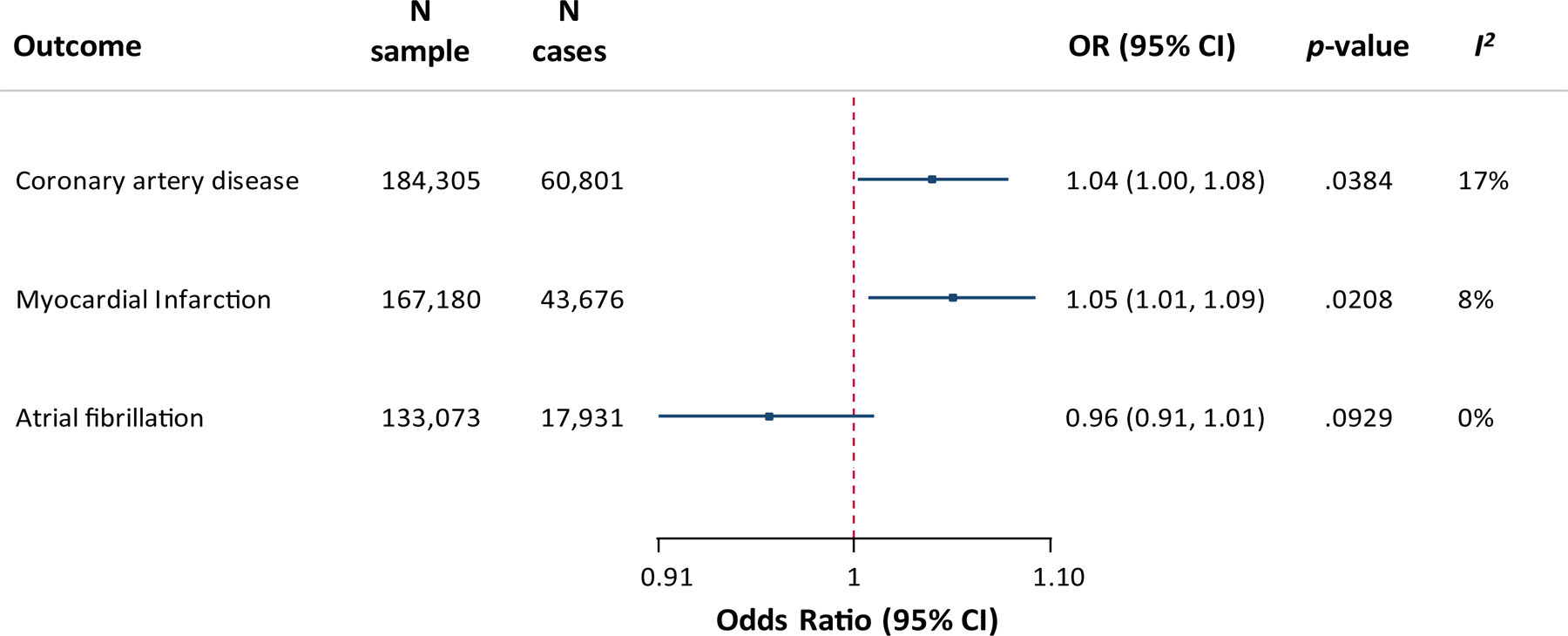
Results: Genetic predisposition to higher MCP-1 levels was associated with higher risk of any stroke (odds ratio [OR] per 1 SD increase, 1.06; 95% CI, 1.02-1.09; P=0.0009), any ischemic stroke (OR, 1.06; 95% CI, 1.02-1.10; P=0.002), large-artery stroke (OR, 1.19; 95% CI, 1.09-1.30; P=0.0002), and cardioembolic stroke (OR, 1.14; 95% CI, 1.06-1.23; P=0.0004), but not with small-vessel stroke or intracerebral hemorrhage. The results were stable in sensitivity analyses and remained significant after adjustment for cardiovascular risk factors. Analyses in the UK Biobank showed similar associations for available phenotypes (any stroke: OR, 1.08; 95% CI, 0.99-1.17; P=0.09; any ischemic stroke: OR, 1.07; 95% CI, 0.97-1.18; P=0.17). Genetically determined higher MCP-1 levels were further associated with coronary artery disease (OR, 1.04; 95% CI, 1.00-1.08; P=0.04) and myocardial infarction (OR, 1.05; 95% CI, 1.01-1.09; P=0.02), but not with atrial fibrillation. A meta-analysis of observational studies showed higher circulating MCP-1 levels in patients with stroke in comparison with controls.
Conclusions: Genetic predisposition to elevated circulating levels of MCP-1 is associated with higher risk of stroke, in particular with large-artery stroke and cardioembolic stroke. Whether targeting MCP-1 or its receptors can lower stroke incidence requires further study.
Keywords: Mendelian randomization analysis; atherosclerosis; chemokine CCL2; cytokines; human genetics; inflammation; stroke.
Figures
Similar articles
-
Genetic associations of adult height with risk of cardioembolic and other subtypes of ischemic stroke: A mendelian randomization study in multiple ancestries.PLoS Med. 2022 Apr 22;19(4):e1003967. doi: 10.1371/journal.pmed.1003967. eCollection 2022 Apr. PLoS Med. 2022. PMID: 35452448 Free PMC article.
-
Genetically proxied appendicular lean mass and stroke risk: A two-step mendelian randomization study.J Stroke Cerebrovasc Dis. 2024 Oct;33(10):107915. doi: 10.1016/j.jstrokecerebrovasdis.2024.107915. Epub 2024 Aug 2. J Stroke Cerebrovasc Dis. 2024. PMID: 39098364
-
The impact of growth differentiation factor 15 on the risk of cardiovascular diseases: two-sample Mendelian randomization study.BMC Cardiovasc Disord. 2020 Oct 28;20(1):462. doi: 10.1186/s12872-020-01744-2. BMC Cardiovasc Disord. 2020. PMID: 33115406 Free PMC article.
-
Circulating Monocyte Chemoattractant Protein-1 and Risk of Stroke: Meta-Analysis of Population-Based Studies Involving 17 180 Individuals.Circ Res. 2019 Sep 27;125(8):773-782. doi: 10.1161/CIRCRESAHA.119.315380. Epub 2019 Sep 3. Circ Res. 2019. PMID: 31476962 Free PMC article.
-
Genome-wide meta-analysis identifies 3 novel loci associated with stroke.Ann Neurol. 2018 Dec;84(6):934-939. doi: 10.1002/ana.25369. Epub 2018 Nov 30. Ann Neurol. 2018. PMID: 30383316 Free PMC article. Review.
Cited by
-
Colchicine for secondary prevention of ischaemic stroke and atherosclerotic events: a meta-analysis of randomised trials.EClinicalMedicine. 2024 Oct 8;76:102835. doi: 10.1016/j.eclinm.2024.102835. eCollection 2024 Oct. EClinicalMedicine. 2024. PMID: 39431112 Free PMC article.
-
Incident Strokes Among American Indian Individuals With Atrial Fibrillation.J Am Heart Assoc. 2021 Mar 16;10(6):e019581. doi: 10.1161/JAHA.120.019581. Epub 2021 Mar 2. J Am Heart Assoc. 2021. PMID: 33653124 Free PMC article.
-
Construction of a Joint Prediction Model for the Occurrence of Ischemic Stroke and Acute Myocardial Infarction Based on Bioinformatic Analysis.Dis Markers. 2022 Apr 4;2022:5967131. doi: 10.1155/2022/5967131. eCollection 2022. Dis Markers. 2022. PMID: 35419117 Free PMC article.
-
Genetics of common cerebral small vessel disease.Nat Rev Neurol. 2022 Feb;18(2):84-101. doi: 10.1038/s41582-021-00592-8. Epub 2022 Jan 5. Nat Rev Neurol. 2022. PMID: 34987231 Review.
-
Revealing brain cell-stratified causality through dissecting causal variants according to their cell-type-specific effects on gene expression.Nat Commun. 2024 Jun 7;15(1):4890. doi: 10.1038/s41467-024-49263-4. Nat Commun. 2024. PMID: 38849352 Free PMC article.
References
-
- Feigin VL, Norrving B and Mensah GA. Global Burden of Stroke. Circ Res. 2017;120:439–448. - PubMed
-
- Esenwa CC and Elkind MS. Inflammatory risk factors, biomarkers and associated therapy in ischaemic stroke. Nat Rev Neurol. 2016;12:594–604. - PubMed
-
- Libby P, Ridker PM and Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473:317–325. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
