

Platelet Serotonin Aggravates Myocardial Ischemia/Reperfusion Injury via Neutrophil Degranulation
- PMID: 30586717
- PMCID: PMC6370531
- DOI: 10.1161/CIRCULATIONAHA.118.033942
Platelet Serotonin Aggravates Myocardial Ischemia/Reperfusion Injury via Neutrophil Degranulation
Abstract
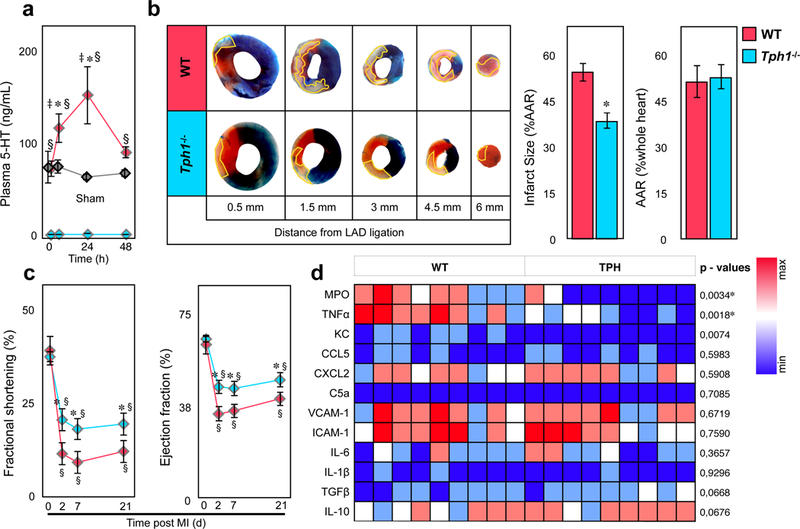
Background: Platelets store large amounts of serotonin that they release during thrombus formation or acute inflammation. This facilitates hemostasis and modulates the inflammatory response.
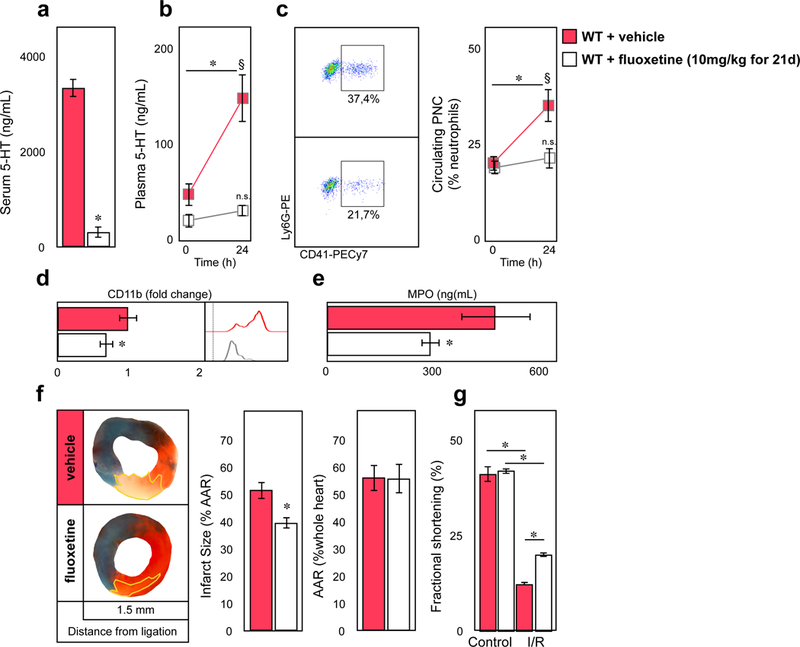
Methods: Infarct size, heart function, and inflammatory cell composition were analyzed in mouse models of myocardial reperfusion injury with genetic and pharmacological depletion of platelet serotonin. These studies were complemented by in vitro serotonin stimulation assays of platelets and leukocytes in mice and men, and by measuring plasma serotonin levels and leukocyte activation in patients with acute coronary syndrome.
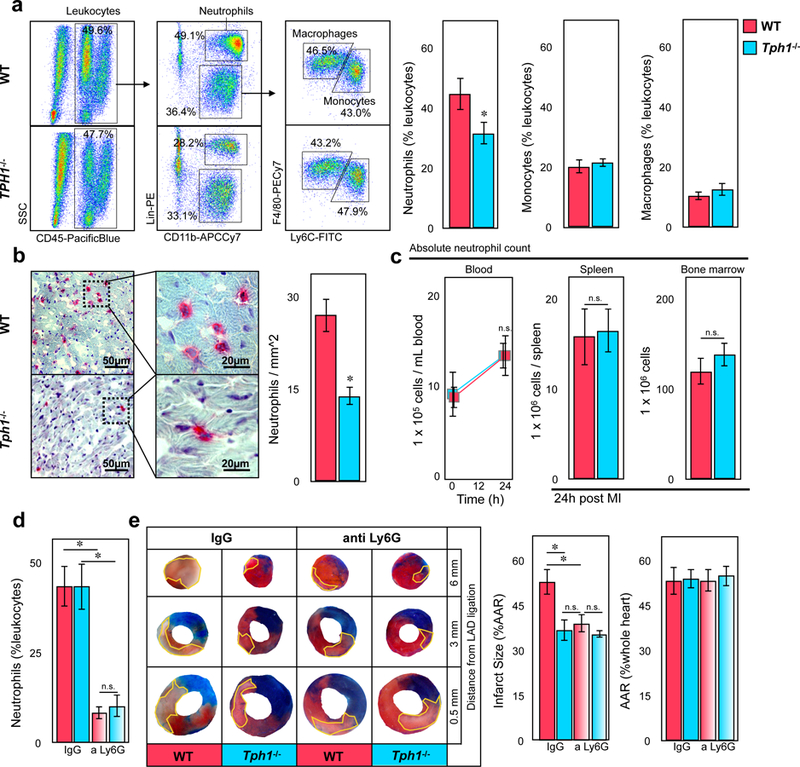
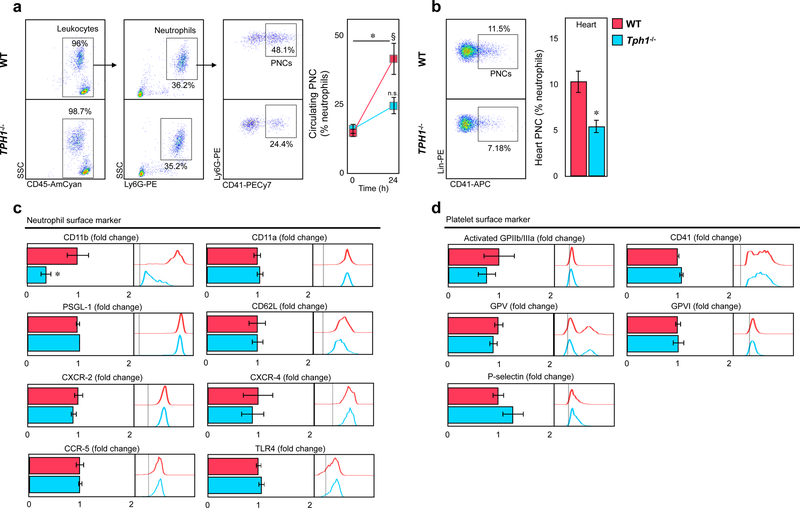
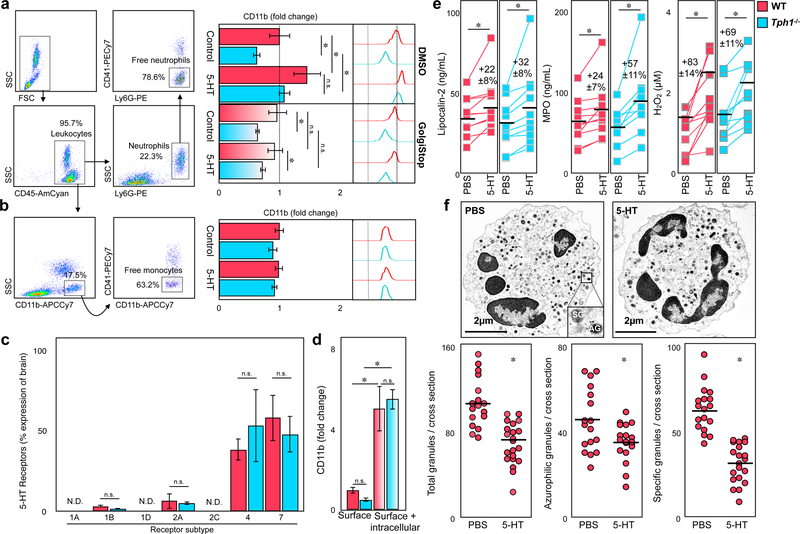
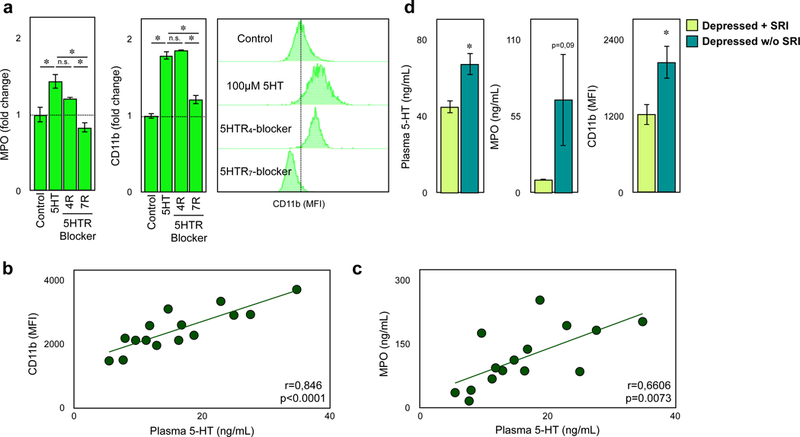
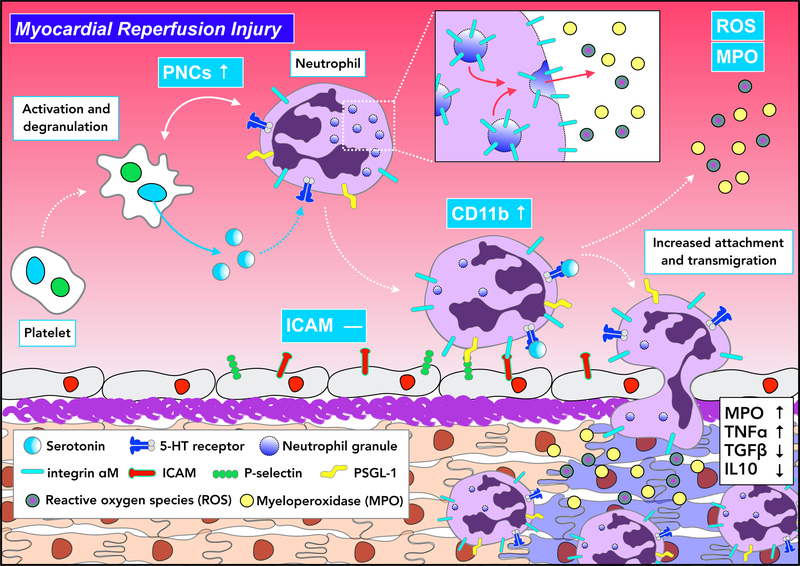
Results: Platelet-derived serotonin induced neutrophil degranulation with release of myeloperoxidase and hydrogen peroxide (H2O2) and increased expression of membrane-bound leukocyte adhesion molecule CD11b, leading to enhanced inflammation in the infarct area and reduced myocardial salvage. In patients hospitalized with acute coronary syndrome, plasmatic serotonin levels correlated with CD11b expression on neutrophils and myeloperoxidase plasma levels. Long-term serotonin reuptake inhibition-reported to protect patients with depression from cardiovascular events-resulted in the depletion of platelet serotonin stores in mice. These mice displayed a reduction in neutrophil degranulation and preserved cardiac function. In line, patients with depression using serotonin reuptake inhibition, presented with suppressed levels of CD11b surface expression on neutrophils and lower myeloperoxidase levels in blood.
Conclusions: Taken together, we identify serotonin as a potent therapeutic target in neutrophil-dependent thromboinflammation during myocardial reperfusion injury.
Keywords: blood platelets; inflammation; integrins; neutrophils; reactive oxygen species; reperfusion injury; serotonin.
Conflict of interest statement
Figures
Comment in
-
Response by Mauler et al to Letter Regarding Article, "Platelet Serotonin Aggravates Myocardial Ischemia/Reperfusion Injury via Neutrophil Degranulation".Circulation. 2019 Aug 13;140(7):e292-e293. doi: 10.1161/CIRCULATIONAHA.119.041481. Epub 2019 Aug 12. Circulation. 2019. PMID: 31403846 No abstract available.
-
Letter by Wang Regarding Article, "Platelet Serotonin Aggravates Myocardial Ischemia/Reperfusion Injury via Neutrophil Degranulation".Circulation. 2019 Aug 13;140(7):e290-e291. doi: 10.1161/CIRCULATIONAHA.119.040803. Epub 2019 Aug 12. Circulation. 2019. PMID: 31403851 No abstract available.
References
-
- Yellon DM and Hausenloy DJ. Myocardial reperfusion injury. N Engl J Med 2007;357:1121–1135. - PubMed
-
- Heusch G and Gersh BJ. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. Eur Heart J 2017;38:774–784. - PubMed
-
- Vinten-Johansen J Involvement of neutrophils in the pathogenesis of lethal myocardial reperfusion injury. Cardiovascular research 2004;61:481–497. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
