

Performance of the ABC Scores for Assessing the Risk of Stroke or Systemic Embolism and Bleeding in Patients With Atrial Fibrillation in ENGAGE AF-TIMI 48
- PMID: 30586727
- PMCID: PMC6363338
- DOI: 10.1161/CIRCULATIONAHA.118.038312
Performance of the ABC Scores for Assessing the Risk of Stroke or Systemic Embolism and Bleeding in Patients With Atrial Fibrillation in ENGAGE AF-TIMI 48
Abstract
Background: The ABC (age, biomarker, clinical history)-stroke and ABC-bleeding risk scores incorporate clinical variables and cardiovascular biomarkers to estimate risk of stroke or systemic embolic events and bleeding, respectively, in patients with atrial fibrillation. These scores have been proposed for routine clinical use, but their performance in external cohorts remains uncertain.
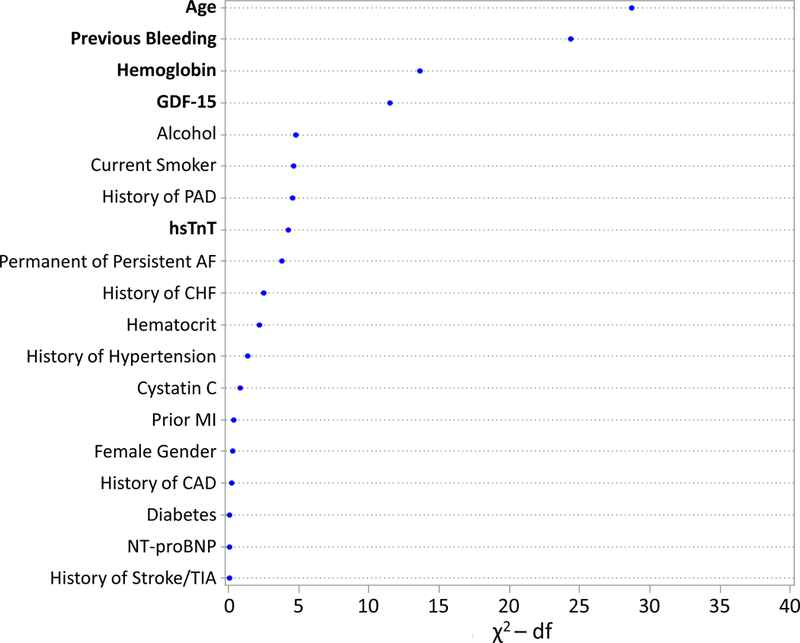
Methods: ENGAGE AF-TIMI 48 (Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48) was a multinational randomized trial of the oral factor Xa inhibitor edoxaban in patients with atrial fibrillation and a CHADS2 score ≥2. We performed a nested prospective biomarker study in 8705 patients, analyzing baseline high-sensitivity troponin T (hsTnT), NT-proBNP (N-terminal B-type natriuretic peptide), and growth differentiation factor-15 (GDF-15), as well as in serial samples after 12 months. The ABC-stroke (age, prior stroke/transient ischemic attack, hsTnT, NT-proBNP) and ABC-bleeding (age, prior bleeding, hemoglobin, hsTnT, and GDF-15) scores were tested. Hazard ratios were adjusted for estimated glomerular filtration rate and the components of the CHA2DS2-VASc and HAS-BLED scores, respectively. Discrimination and reclassification were compared with these established scores.
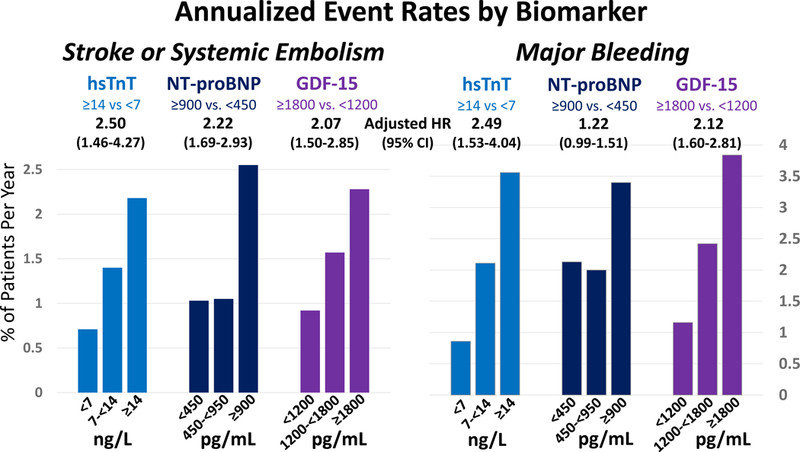
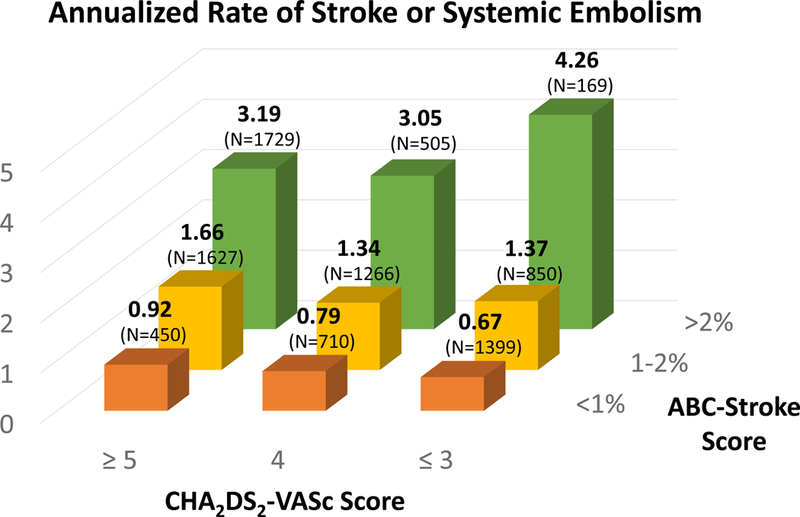
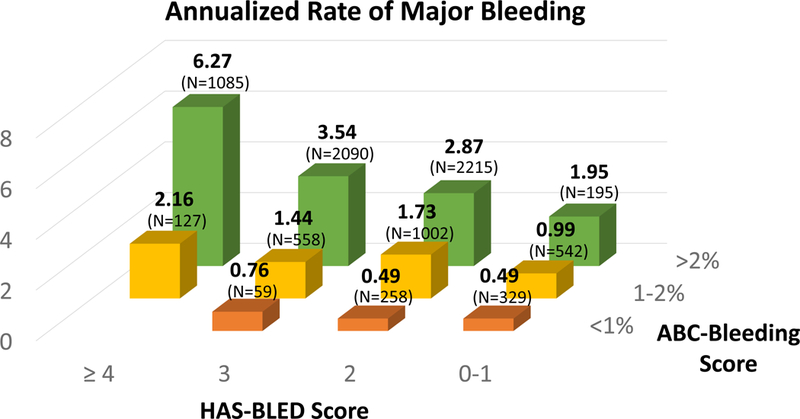
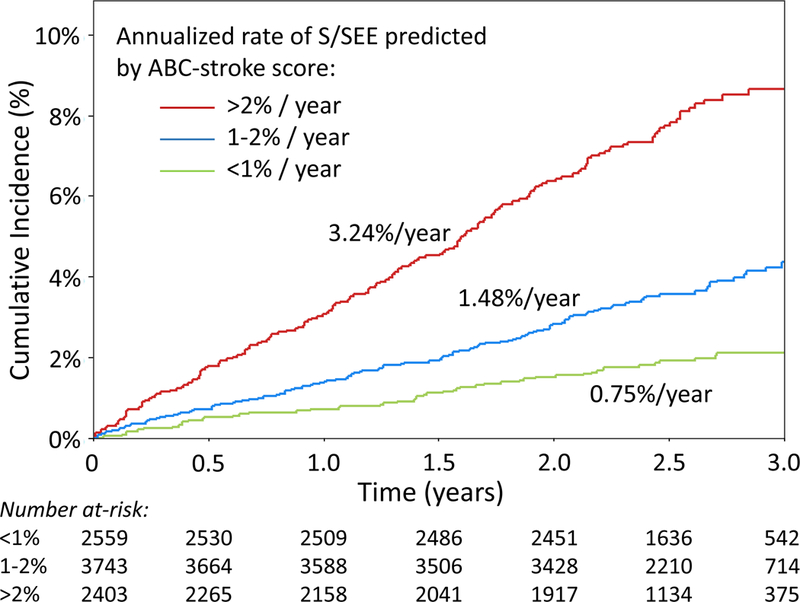
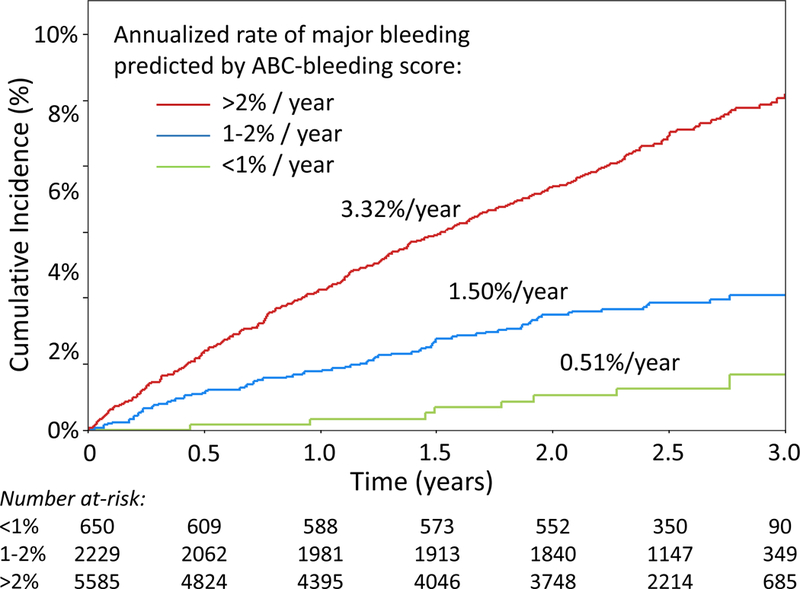
Results: Median baseline hsTnT, NT-proBNP, and GDF-15 levels were 13.7 ng/L (25th-75th percentiles, 9.6-20.4 ng/L), 811 pg/mL (386-1436 pg/mL), and 1661 pg/mL (1179-2427 pg/mL), respectively. Elevated hsTnT, NT-proBNP, and GDF-15 were independently associated with higher rates of stroke or systemic embolic events, and elevated hsTnT and GDF-15 were independently associated with higher rates of major bleeding ( P<0.001 for each). The ABC-stroke and ABC-bleeding scores were well calibrated and yielded higher c indexes than the CHA2DS2-VASc score for stroke or systemic embolic events (0.67 [95% CI, 0.65-0.70] versus 0.59 [95% CI, 0.57-0.62]; P<0.001) and HAS-BLED score for major bleeding (0.69 [95% CI, 0.66-0.71] versus 0.62 [95% CI, 0.60-0.64]; P<0.001), respectively. The ABC-stroke and ABC-bleeding scores stratified patients within CHA2DS2-VASc and HAS-BLED risk categories ( P<0.001 for both). Patients with ABC-bleeding scores predicting a high 1-year risk of bleeding (>2%) derived greater benefit from treatment with edoxaban compared with warfarin.
Conclusions: The ABC-stroke and ABC-bleeding scores evaluated in this anticoagulated clinical trial cohort were well calibrated and outperformed the CHA2DS2-VASc and HAS-BLED scores, respectively. These scores may help identify patients most likely to derive a benefit from treatment with non-vitamin K antagonist oral anticoagulants.
Clinical trial registration: URL: https://www.clinicaltrials.gov . Unique identifier: NCT00781391.
Keywords: atrial fibrillation; biomarkers; hemorrhage; risk assessment; stroke.
Figures

Comment in
-
Biomarkers for Prediction of Stroke and Bleeds in Atrial Fibrillation.Circulation. 2019 Feb 5;139(6):772-774. doi: 10.1161/CIRCULATIONAHA.118.038635. Circulation. 2019. PMID: 30715942 No abstract available.
-
In AF, ABC scores predicted stroke or major bleeding better than CHA2DS2-VASc and HAS-BLED scores, respectively.Ann Intern Med. 2019 Jun 18;170(12):JC71. doi: 10.7326/ACPJ201906180-071. Ann Intern Med. 2019. PMID: 31207624 No abstract available.
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017;135:e146–e603. - PMC - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr., Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW and Members AATF. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014;130:2071–2104. - PubMed
-
- Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, Haeusler KG, Oldgren J, Reinecke H, Roldan-Schilling V, Rowell N, Sinnaeve P, Collins R, Camm AJ, Heidbuchel H and Group ESCSD. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J 2018;39:1330–1393. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL and Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace 2016;18:1609–1678. - PubMed
-
- Wilke T, Groth A, Mueller S, Pfannkuche M, Verheyen F, Linder R, Maywald U, Kohlmann T, Feng YS, Breithardt G and Bauersachs R. Oral anticoagulation use by patients with atrial fibrillation in Germany. Adherence to guidelines, causes of anticoagulation under-use and its clinical outcomes, based on claims-data of 183,448 patients. Thromb Haemost 2012;107:1053–1065. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
