

Myocardial and Systemic Inflammation in Acute Stress-Induced (Takotsubo) Cardiomyopathy
- PMID: 30586731
- PMCID: PMC6438459
- DOI: 10.1161/CIRCULATIONAHA.118.037975
Myocardial and Systemic Inflammation in Acute Stress-Induced (Takotsubo) Cardiomyopathy
Abstract
Background: Acute stress-induced (takotsubo) cardiomyopathy can result in a heart failure phenotype with a prognosis comparable with that of myocardial infarction. In this study, we hypothesized that inflammation is central to the pathophysiology and natural history of takotsubo cardiomyopathy.
Methods: In a multicenter study, we prospectively recruited 55 patients with takotsubo cardiomyopathy and 51 age-, sex-, and comorbidity-matched control subjects. During the index event and at the 5-month follow-up, patients with takotsubo cardiomyopathy underwent multiparametric cardiac magnetic resonance imaging, including ultrasmall superparamagnetic particles of iron oxide (USPIO) enhancement for detection of inflammatory macrophages in the myocardium. Blood monocyte subpopulations and serum cytokines were assessed as measures of systemic inflammation. Matched control subjects underwent investigation at a single time point.
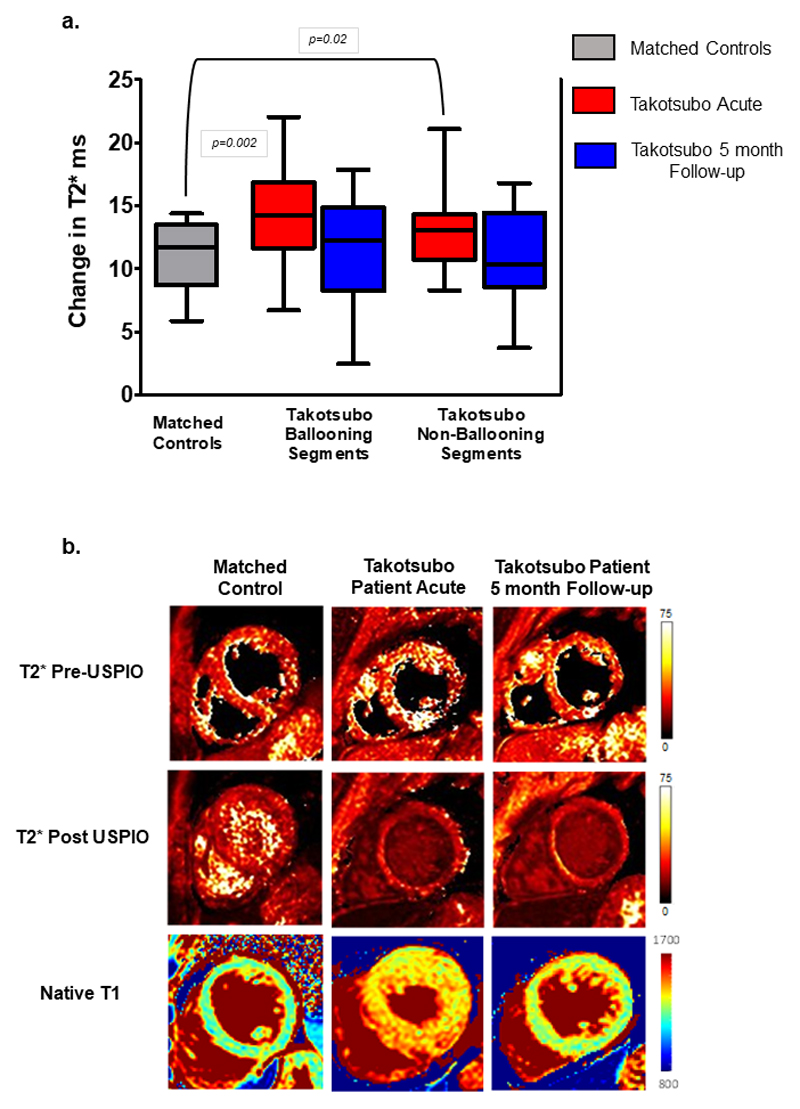
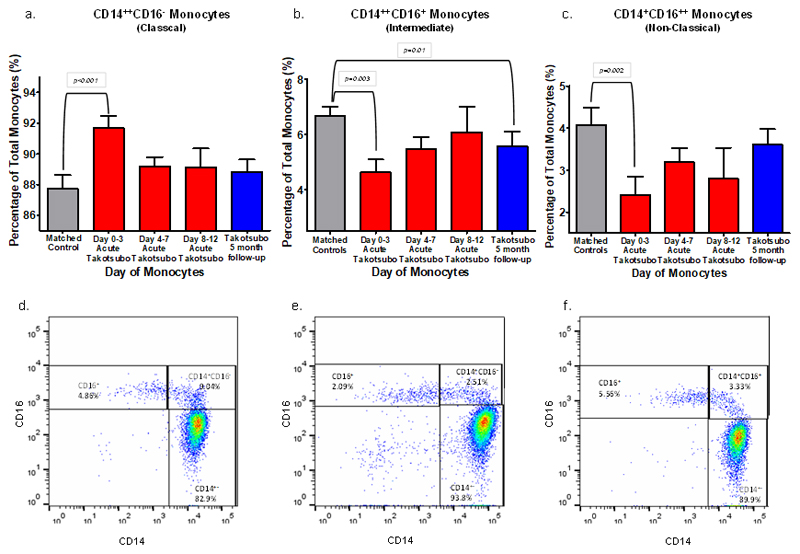
Results: Subjects were predominantly middle-aged (64±14 years) women (90%). Compared with control subjects, patients with takotsubo cardiomyopathy had greater USPIO enhancement (expressed as the difference between pre-USPIO and post-USPIO T2*) in both ballooning (14.3±0.6 milliseconds versus 10.5±0.9 milliseconds; P<0.001) and nonballooning (12.9±0.6 milliseconds versus 10.5±0.9 milliseconds; P=0.02) left ventricular myocardial segments. Serum interleukin-6 (23.1±4.5 pg/mL versus 6.5±5.8 pg/mL; P<0.001) and chemokine (C-X-C motif) ligand 1 (1903±168 pg/mL versus 1272±177 pg/mL; P=0.01) concentrations and classic CD14++CD16- monocytes (90±0.5% versus 87±0.9%; P=0.01) were also increased whereas intermediate CD14++CD16+ (5.4±0.3% versus 6.9±0.6%; P=0.01) and nonclassic CD14+CD16++ (2.7±0.3% versus 4.2±0.5%; P=0.006) monocytes were reduced in patients with takotsubo cardiomyopathy. At 5 months, USPIO enhancement was no longer detectable in the left ventricular myocardium, although persistent elevations in serum interleukin-6 concentrations ( P=0.009) and reductions in intermediate CD14++CD16+ monocytes (5.6±0.4% versus 6.9±0.6%; P=0.01) remained.
Conclusions: We demonstrate for the first time that takotsubo cardiomyopathy is characterized by a myocardial macrophage inflammatory infiltrate, changes in the distribution of monocyte subsets, and an increase in systemic proinflammatory cytokines. Many of these changes persisted for at least 5 months, suggesting a low-grade chronic inflammatory state.
Clinical trial registration: URL: https://www.clinicaltrials.gov . Unique identifier: NCT02897739.
Keywords: cardiomyopathies; cytokines; inflammation; macrophages; monocytes; takotsubo cardiomyopathy; ultrasmall superparamagnetic iron oxide particles (USPIO).
Conflict of interest statement
Figures
Comment in
-
Inflammation linked to Takotsubo.Nat Rev Cardiol. 2019 Jan;16(1):5. doi: 10.1038/s41569-018-0128-3. Nat Rev Cardiol. 2019. PMID: 30479385 No abstract available.
-
Response by Scally and Dawson to Letters Regarding Article, "Myocardial and Systemic Inflammation in Acute Stress-Induced (Takotsubo) Cardiomyopathy".Circulation. 2019 Sep 24;140(13):e698-e699. doi: 10.1161/CIRCULATIONAHA.119.041878. Epub 2019 Sep 23. Circulation. 2019. PMID: 31545684 No abstract available.
-
Letter by Tajiri et al Regarding Article, "Myocardial and Systemic Inflammation in Acute Stress-Induced (Takotsubo) Cardiomyopathy".Circulation. 2019 Sep 24;140(13):e694-e695. doi: 10.1161/CIRCULATIONAHA.119.041319. Epub 2019 Sep 23. Circulation. 2019. PMID: 31545687 No abstract available.
-
Letter by Khalid et al Regarding Article, "Myocardial and Systemic Inflammation in Acute Stress-Induced (Takotsubo) Cardiomyopathy".Circulation. 2019 Sep 24;140(13):e696-e697. doi: 10.1161/CIRCULATIONAHA.118.039463. Epub 2019 Sep 23. Circulation. 2019. PMID: 31545688 No abstract available.
References
-
- Redfors B, Vedad R, Angeras O, Ramunddal T, Petursson P, Haraldsson I, Ali A, Dworeck C, Odenstedt J, Ioaness D, Libungan B, et al. Mortality in takotsubo syndrome is similar to mortality in myocardial infarction - A report from the SWEDEHEART registry. Int J Cardiol. 2015;185:282–289. - PubMed
-
- Brinjikji W, El-Sayed AM, Salka S. In-hospital mortality among patients with takotsubo cardiomyopathy: a study of the National Inpatient Sample 2008 to 2009. Am Heart J. 2012;164:215–221. - PubMed
-
- Tornvall P, Collste O, Ehrenborg E, Jarnbert-Petterson H. A Case-Control Study of Risk Markers and Mortality in Takotsubo Stress Cardiomyopathy. J Am Coll Cardiol. 2016;67:1931–1936. - PubMed
-
- Dawson DK, Neil CJ, Henning A, Cameron D, Jagpal B, Bruce M, Horowitz J, Frenneaux MP. Tako-Tsubo Cardiomyopathy: A Heart Stressed Out of Energy? Jacc-Cardiovascular Imaging. 2015;8:985–987. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
