

Whole-Genome Sequencing to Characterize Monogenic and Polygenic Contributions in Patients Hospitalized With Early-Onset Myocardial Infarction
- PMID: 30586733
- PMCID: PMC6433484
- DOI: 10.1161/CIRCULATIONAHA.118.035658
Whole-Genome Sequencing to Characterize Monogenic and Polygenic Contributions in Patients Hospitalized With Early-Onset Myocardial Infarction
Abstract
Background: The relative prevalence and clinical importance of monogenic mutations related to familial hypercholesterolemia and of high polygenic score (cumulative impact of many common variants) pathways for early-onset myocardial infarction remain uncertain. Whole-genome sequencing enables simultaneous ascertainment of both monogenic mutations and polygenic score for each individual.
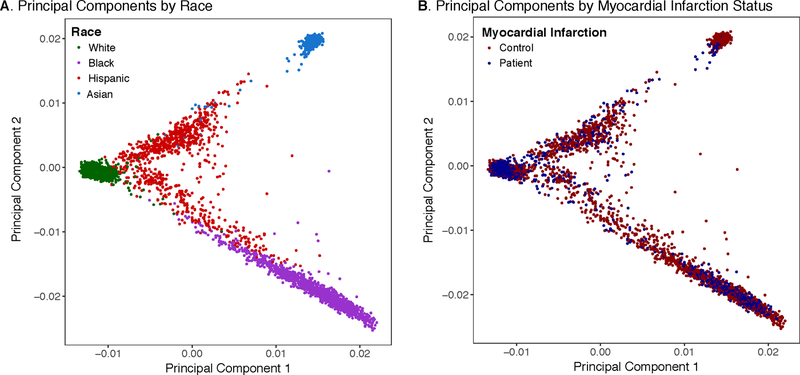
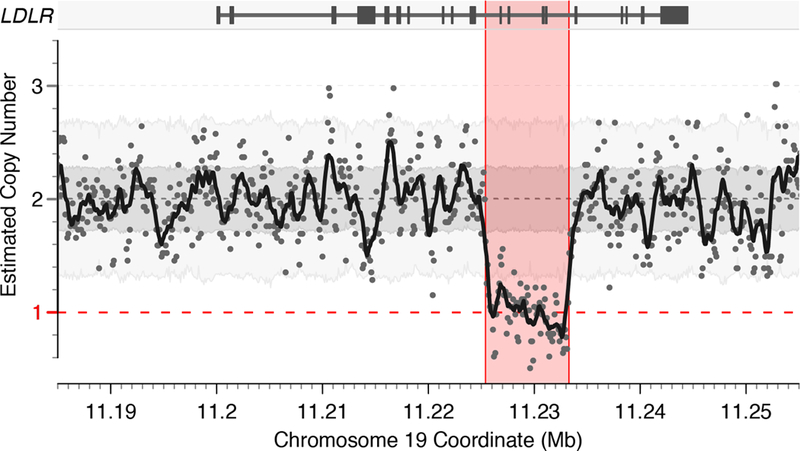
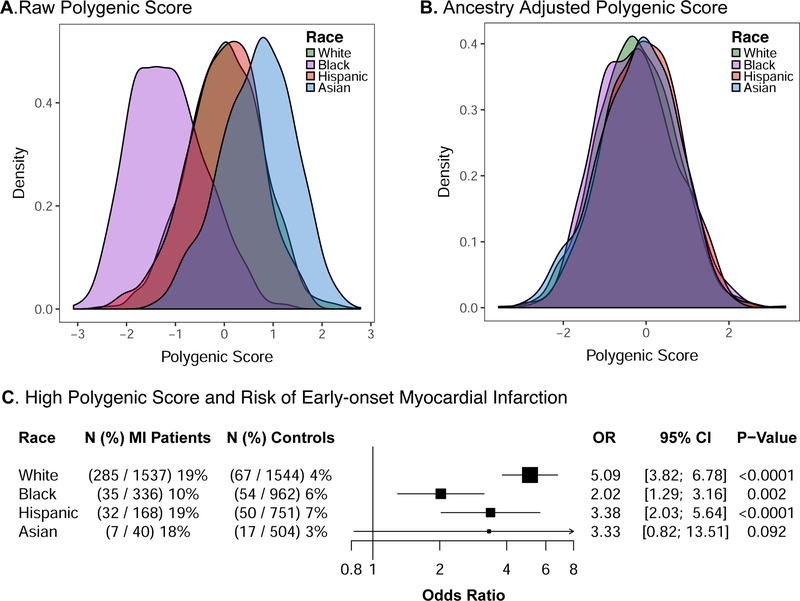
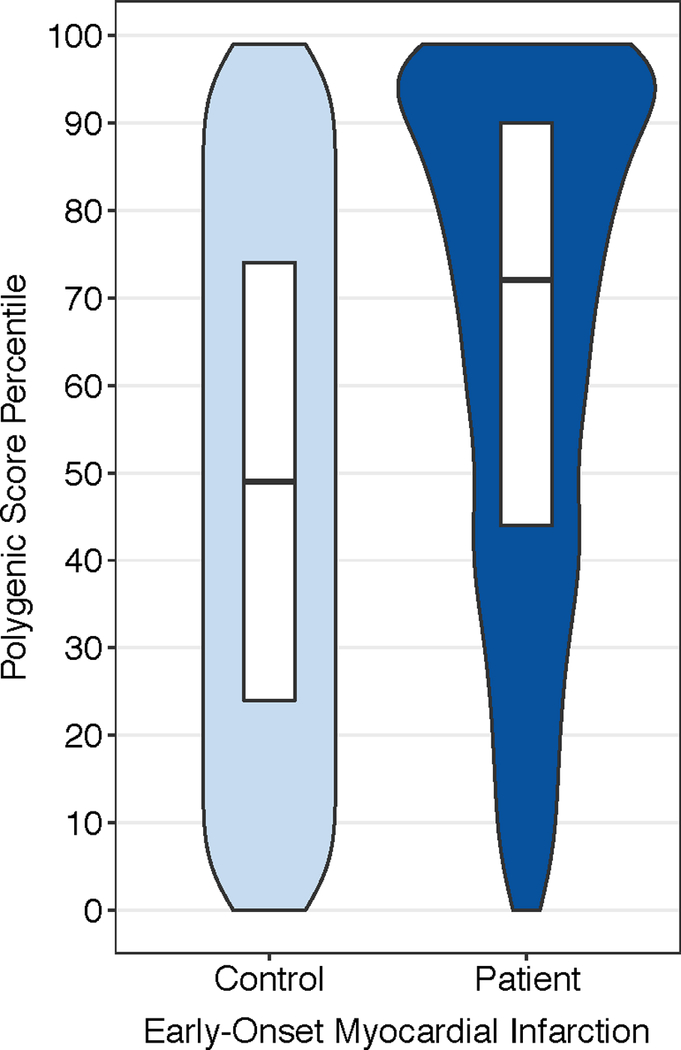
Methods: We performed deep-coverage whole-genome sequencing of 2081 patients from 4 racial subgroups hospitalized in the United States with early-onset myocardial infarction (age ≤55 years) recruited with a 2:1 female-to-male enrollment design. We compared these genomes with those of 3761 population-based control subjects. We first identified individuals with a rare, monogenic mutation related to familial hypercholesterolemia. Second, we calculated a recently developed polygenic score of 6.6 million common DNA variants to quantify the cumulative susceptibility conferred by common variants. We defined high polygenic score as the top 5% of the control distribution because this cutoff has previously been shown to confer similar risk to that of familial hypercholesterolemia mutations.
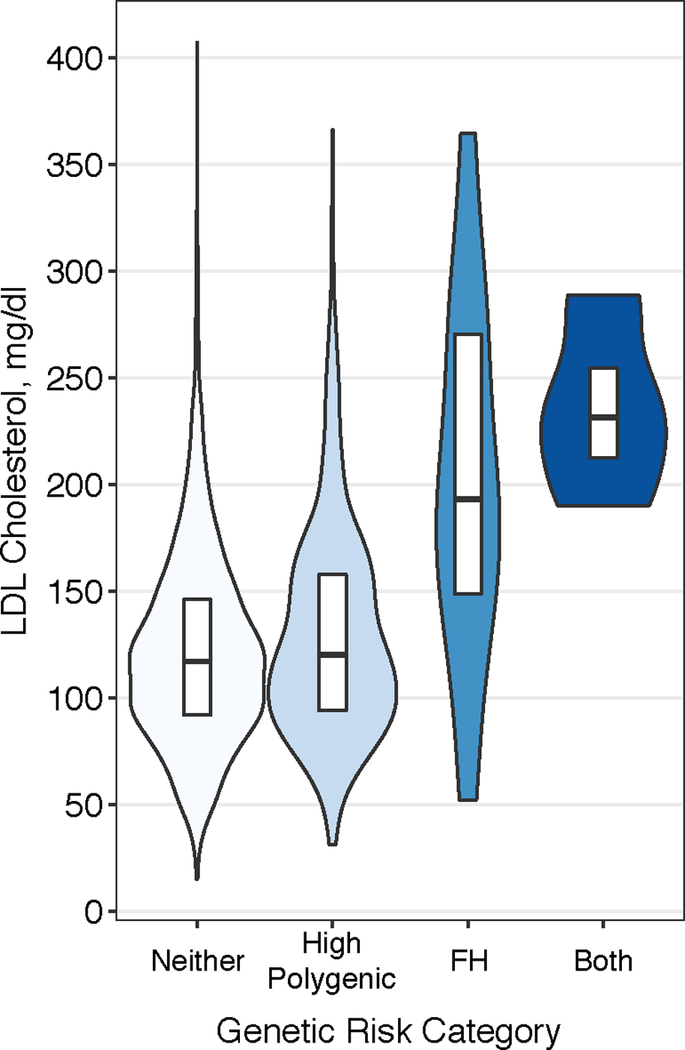
Results: The mean age of the 2081 patients presenting with early-onset myocardial infarction was 48 years, and 66% were female. A familial hypercholesterolemia mutation was present in 36 of these patients (1.7%) and was associated with a 3.8-fold (95% CI, 2.1-6.8; P<0.001) increased odds of myocardial infarction. Of the patients with early-onset myocardial infarction, 359 (17.3%) carried a high polygenic score, associated with a 3.7-fold (95% CI, 3.1-4.6; P<0.001) increased odds. Mean estimated untreated low-density lipoprotein cholesterol was 206 mg/dL in those with a familial hypercholesterolemia mutation, 132 mg/dL in those with high polygenic score, and 122 mg/dL in those in the remainder of the population. Although associated with increased risk in all racial groups, high polygenic score demonstrated the strongest association in white participants ( P for heterogeneity=0.008).
Conclusions: Both familial hypercholesterolemia mutations and high polygenic score are associated with a >3-fold increased odds of early-onset myocardial infarction. However, high polygenic score has a 10-fold higher prevalence among patients presents with early-onset myocardial infarction.
Clinical trial registration: URL: https://www.clinicaltrials.gov . Unique identifier: NCT00597922.
Keywords: genetics; humans; hypercholesterolemia; myocardial infarction; risk.
Figures
References
-
- Gertler MM, Garn SM and White PD. Young candidates for coronary heart disease. J Am Med Assoc 1951;147:621–625. - PubMed
-
- Do R, Stitziel NO, Won HH, Jorgensen AB, Duga S, Angelica Merlini P, Kiezun A, Farrall M, Goel A, Zuk O, Guella I, Asselta R, Lange LA, Peloso GM, Auer PL, Girelli D, Martinelli N, Farlow DN, DePristo MA, Roberts R, Stewart AF, Saleheen D, Danesh J, Epstein SE, Sivapalaratnam S, Hovingh GK, Kastelein JJ, Samani NJ, Schunkert H, Erdmann J, Shah SH, Kraus WE, Davies R, Nikpay M, Johansen CT, Wang J, Hegele RA, Hechter E, Marz W, Kleber ME, Huang J, Johnson AD, Li M, Burke GL, Gross M, Liu Y, Assimes TL, Heiss G, Lange EM, Folsom AR, Taylor HA, Olivieri O, Hamsten A, Clarke R, Reilly DF, Yin W, Rivas MA, Donnelly P, Rossouw JE, Psaty BM, Herrington DM, Wilson JG, Rich SS, Bamshad MJ, Tracy RP, Cupples LA, Rader DJ, Reilly MP, Spertus JA, Cresci S, Hartiala J, Tang WH, Hazen SL, Allayee H, Reiner AP, Carlson CS, Kooperberg C, Jackson RD, Boerwinkle E, Lander ES, Schwartz SM, Siscovick DS, McPherson R, Tybjaerg-Hansen A, Abecasis GR, Watkins H, Nickerson DA, Ardissino D, Sunyaev SR, O’Donnell CJ, Altshuler D, Gabriel S and Kathiresan S. Exome sequencing identifies rare LDLR and APOA5 alleles conferring risk for myocardial infarction. Nature 2015;518:102–106. - PMC - PubMed
-
- Khera AV, Won HH, Peloso GM, Lawson KS, Bartz TM, Deng X, van Leeuwen EM, Natarajan P, Emdin CA, Bick AG, Morrison AC, Brody JA, Gupta N, Nomura A, Kessler T, Duga S, Bis JC, van Duijn CM, Cupples LA, Psaty B, Rader DJ, Danesh J, Schunkert H, McPherson R, Farrall M, Watkins H, Lander E, Wilson JG, Correa A, Boerwinkle E, Merlini PA, Ardissino D, Saleheen D, Gabriel S and Kathiresan S. Diagnostic Yield and Clinical Utility of Sequencing Familial Hypercholesterolemia Genes in Patients With Severe Hypercholesterolemia. J Am Coll Cardiol 2016;67:2578–2589. - PMC - PubMed
-
- Benn M, Watts GF, Tybjaerg-Hansen A and Nordestgaard BG. Mutations causative of familial hypercholesterolaemia: screening of 98 098 individuals from the Copenhagen General Population Study estimated a prevalence of 1 in 217. Eur Heart J 2016;37:1384–94. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- KL2 TR001100/TR/NCATS NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- T32 HG002295/HG/NHGRI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL105756/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- R01 HL081153/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- UM1 HG008895/HG/NHGRI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- R01 HL127564/HL/NHLBI NIH HHS/United States
- T32 HL007208/HL/NHLBI NIH HHS/United States
- R01 HL142711/HL/NHLBI NIH HHS/United States
- T32 GM007205/GM/NIGMS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- K08 HG010155/HG/NHGRI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
