

Phase I/II Trial of Electrophysiology-Guided Noninvasive Cardiac Radioablation for Ventricular Tachycardia
- PMID: 30586734
- PMCID: PMC6331281
- DOI: 10.1161/CIRCULATIONAHA.118.038261
Phase I/II Trial of Electrophysiology-Guided Noninvasive Cardiac Radioablation for Ventricular Tachycardia
Abstract
Background: Case studies have suggested the efficacy of catheter-free, electrophysiology-guided noninvasive cardiac radioablation for ventricular tachycardia (VT) using stereotactic body radiation therapy, although prospective data are lacking.
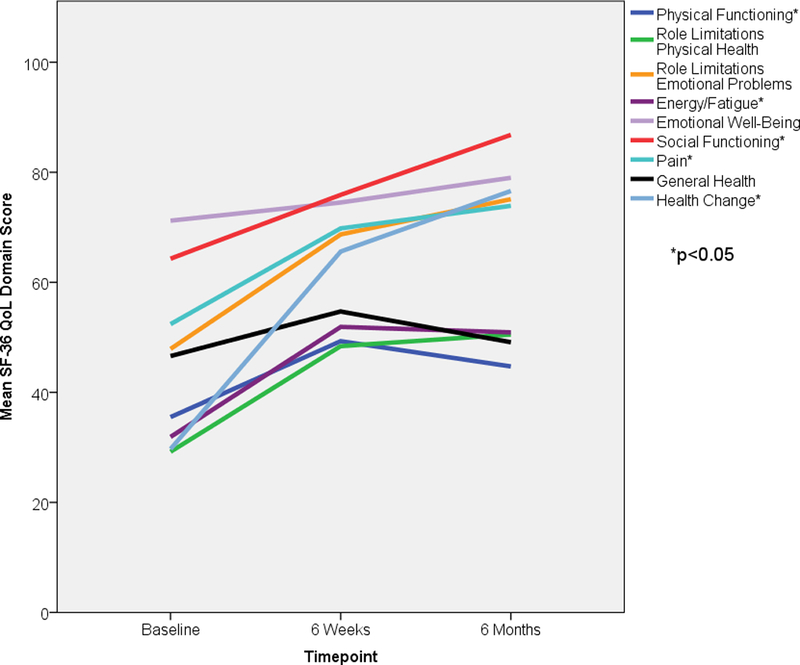
Methods: We conducted a prospective phase I/II trial of noninvasive cardiac radioablation in adults with treatment-refractory episodes of VT or cardiomyopathy related to premature ventricular contractions (PVCs). Arrhythmogenic scar regions were targeted by combining noninvasive anatomic and electric cardiac imaging with a standard stereotactic body radiation therapy workflow followed by delivery of a single fraction of 25 Gy to the target. The primary safety end point was treatment-related serious adverse events in the first 90 days. The primary efficacy end point was any reduction in VT episodes (tracked by indwelling implantable cardioverter defibrillators) or any reduction in PVC burden (as measured by a 24-hour Holter monitor) comparing the 6 months before and after treatment (with a 6-week blanking window after treatment). Health-related quality of life was assessed using the Short Form-36 questionnaire.
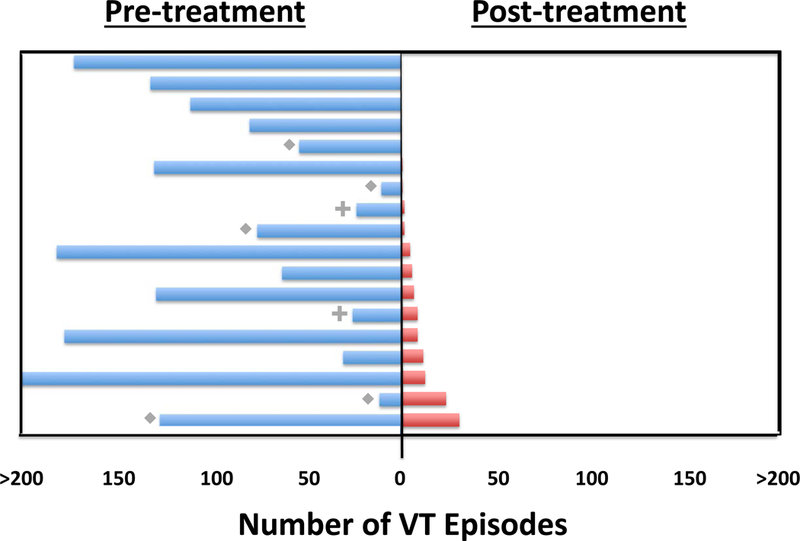
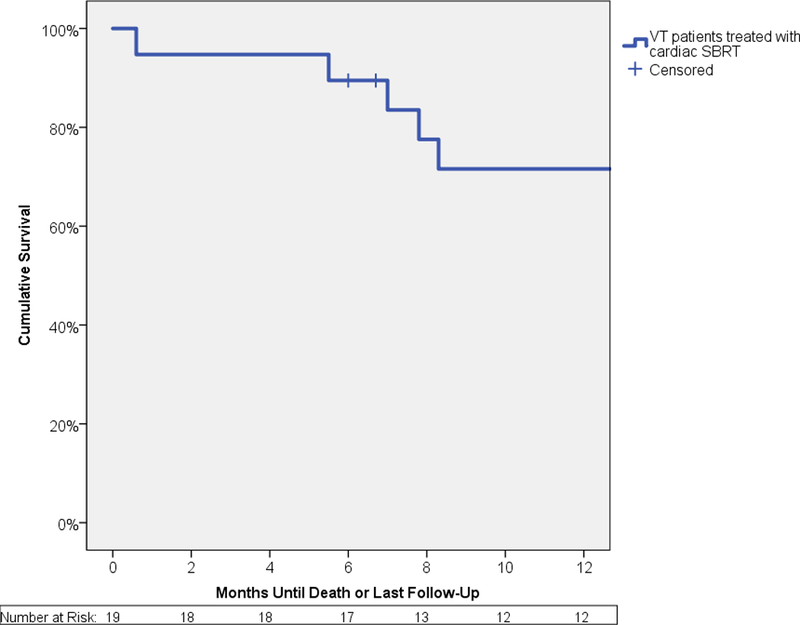
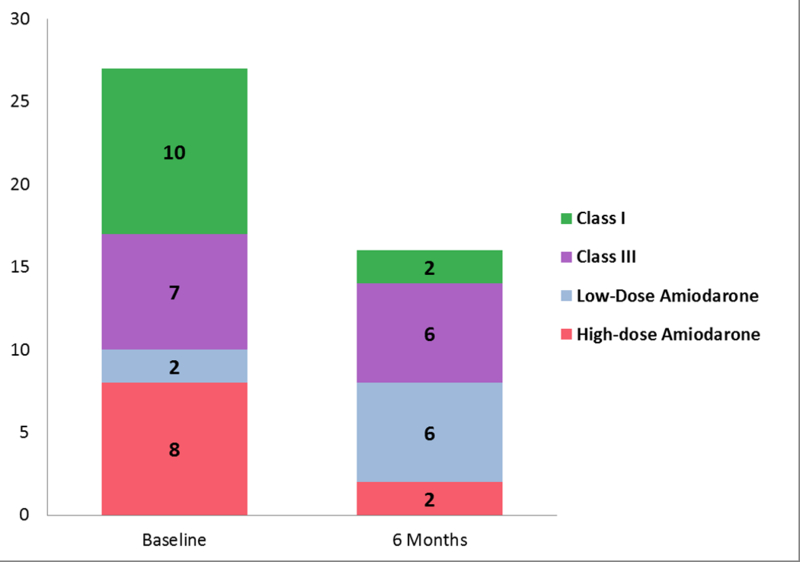
Results: Nineteen patients were enrolled (17 for VT, 2 for PVC cardiomyopathy). Median noninvasive ablation time was 15.3 minutes (range, 5.4-32.3). In the first 90 days, 2/19 patients (10.5%) developed a treatment-related serious adverse event. The median number of VT episodes was reduced from 119 (range, 4-292) to 3 (range, 0-31; P<0.001). Reduction was observed for both implantable cardioverter defibrillator shocks and antitachycardia pacing. VT episodes or PVC burden were reduced in 17/18 evaluable patients (94%). The frequency of VT episodes or PVC burden was reduced by 75% in 89% of patients. Overall survival was 89% at 6 months and 72% at 12 months. Use of dual antiarrhythmic medications decreased from 59% to 12% ( P=0.008). Quality of life improved in 5 of 9 Short Form-36 domains at 6 months.
Conclusions: Noninvasive electrophysiology-guided cardiac radioablation is associated with markedly reduced ventricular arrhythmia burden with modest short-term risks, reduction in antiarrhythmic drug use, and improvement in quality of life.
Clinical trial registration: URL: https://www.clinicaltrials.gov/ . Unique identifier: NCT02919618.
Keywords: noninvasive; stereotactic radiotherapy; ventricular tachycardia.
Figures
Comment in
-
Noninvasive Stereotactic Radioablation for Ventricular Tachycardia.Circulation. 2019 Jan 15;139(3):322-324. doi: 10.1161/CIRCULATIONAHA.118.038285. Circulation. 2019. PMID: 30586783 No abstract available.
-
Response by Robinson et al to Letter Regarding Article, "Phase I/II Trial of Electrophysiology-Guided Noninvasive Cardiac Radioablation for Ventricular Tachycardia".Circulation. 2019 Jul 2;140(1):e3-e4. doi: 10.1161/CIRCULATIONAHA.119.040793. Epub 2019 Jul 1. Circulation. 2019. PMID: 31549873 No abstract available.
-
Letter by Jumeau et al Regarding Article, "Phase I/II Trial of Electrophysiology-Guided Noninvasive Cardiac Radioablation for Ventricular Tachycardia".Circulation. 2019 Jul 2;140(1):e1-e2. doi: 10.1161/CIRCULATIONAHA.118.039019. Epub 2019 Jul 1. Circulation. 2019. PMID: 31549874 No abstract available.
References
-
- Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, Deal BJ, Dickfeld T, Field ME, Fonarow GC, Gillis AM, Hlatky MA, Granger CB, Hammill SC, Joglar JA, Kay GN, Matlock DD, Myerburg RJ and Page RL. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;138:e272–e391. - PubMed
-
- Dukkipati SR, Koruth JS, Choudry S, Miller MA, Whang W and Reddy VY. Catheter Ablation of Ventricular Tachycardia in Structural Heart Disease: Indications, Strategies, and Outcomes-Part II. J Am Coll Cardiol. 2017;70:2924–2941. - PubMed
-
- Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, Keall P, Lovelock M, Meeks S, Papiez L, Purdie T, Sadagopan R, Schell MC, Salter B, Schlesinger DJ, Shiu AS, Solberg T, Song DY, Stieber V, Timmerman R, Tome WA, Verellen D, Wang L and Yin FF. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010;37:4078–4101. - PubMed
-
- Roach MC, Robinson CG, DeWees TA, Ganachaud J, Przybysz D, Drzymala R, Rehman S, Kashani R and Bradley JD. Stereotactic Body Radiation Therapy for Central Early-Stage NSCLC: Results of a Prospective Phase I/II Trial. J Thorac Oncol. 2018. doi: 10.1016/j.jtho.2018.07.017. [Epub ahead of print] - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
