

Quantifying Importance of Major Risk Factors for Coronary Heart Disease
- PMID: 30586759
- PMCID: PMC6433489
- DOI: 10.1161/CIRCULATIONAHA.117.031855
Quantifying Importance of Major Risk Factors for Coronary Heart Disease
Abstract
Background: To optimize preventive strategies for coronary heart disease (CHD), it is essential to understand and appropriately quantify the contribution of its key risk factors. Our objective was to compare the associations of key modifiable CHD risk factors-specifically lipids, systolic blood pressure (SBP), diabetes mellitus, and smoking-with incident CHD events based on their prognostic performance, attributable risk fractions, and treatment benefits, overall and by age.
Methods: Pooled participant-level data from 4 observational cohort studies sponsored by the National Heart, Lung, and Blood Institute were used to create a cohort of 22 626 individuals aged 45 to 84 years who were initially free of cardiovascular disease. Individuals were followed for 10 years from baseline evaluation for incident CHD. Proportional hazards regression was used to estimate metrics of prognostic model performance (likelihood ratio, C index, net reclassification, discrimination slope), hazard ratios, and population attributable fractions for SBP, non-high-density lipoprotein cholesterol (non-HDL-C), diabetes mellitus, and smoking. Expected absolute risk reductions for antihypertensive and lipid-lowering treatment were assessed.
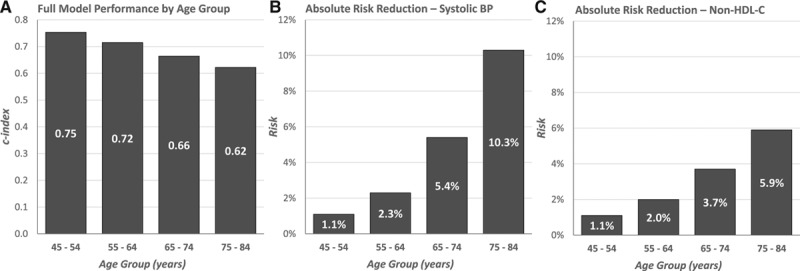
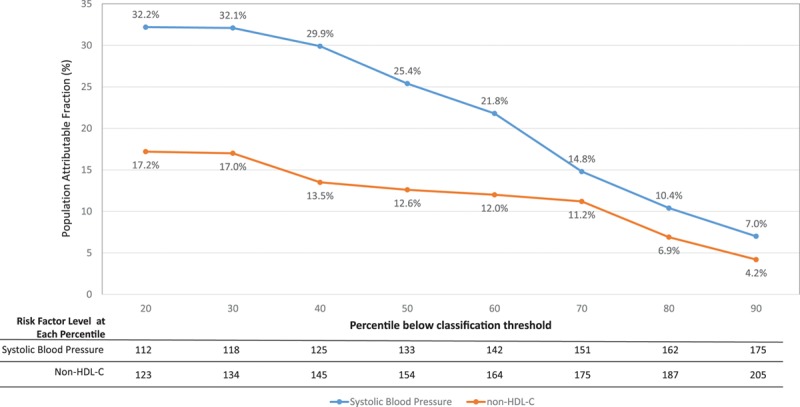
Results: Age, sex, and race capture 63% to 80% of the prognostic performance of cardiovascular risk models. In contrast, adding either SBP, non-HDL-C, diabetes mellitus, or smoking to a model with other risk factors increases the C index by only 0.004 to 0.013. However, primordial prevention could have a substantial effect as demonstrated by population attributable fractions of 28% for SBP≥130 mm Hg and 17% for non-HDL-C≥130 mg/dL. Similarly, lowering the SBP of all individuals to <130 mm Hg or lowering low-density lipoprotein cholesterol by 30% would be expected to lower a baseline 10-year CHD risk of 10.7% to 7.0 and 8.0, respectively (absolute risk reductions: 3.7% and 2.7%, respectively). Prognostic performance decreases with age (C indices for age groups 45-54, 55-64, 65-74, 75-84 are 0.75, 0.72, 0.66, and 0.62, respectively), whereas absolute risk reductions increase (SBP: 1.1%, 2.3%, 5.4%, 10.3%, respectively; non-HDL-C: 1.1%, 2.0%, 3.7%, 5.9%, respectively).
Conclusions: Although individual modifiable CHD risk factors contribute only modestly to prognostic performance, our models indicate that eliminating or controlling these individual factors would lead to substantial reductions in total population CHD events. Metrics used to judge importance of risk factors should be tailored to the research objectives.
Keywords: blood pressure; cholesterol, LDL; coronary disease; lipoproteins, HDL2; population; risk factors.
Figures
References
-
- Wang TJ, Gona P, Larson MG, Tofler GH, Levy D, Newton-Cheh C, Jacques PF, Rifai N, Selhub J, Robins SJ, Benjamin EJ, D’Agostino RB, Vasan RS. Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med. 2006;355:2631–2639. doi: 10.1056/NEJMoa055373. - PubMed
-
- Laaksonen MA, Knekt P, Rissanen H, Härkänen T, Virtala E, Marniemi J, Aromaa A, Heliövaara M, Reunanen A. The relative importance of modifiable potential risk factors of type 2 diabetes: a meta-analysis of two cohorts. Eur J Epidemiol. 2010;25:115–124. doi: 10.1007/s10654-009-9405-0. - PubMed
-
- Thanassoulis G, Williams K, Altobelli KK, Pencina MJ, Cannon CP, Sniderman AD. Individualized statin benefit for determining statin eligibility in the primary prevention of cardiovascular disease. Circulation. 2016;133:1574–1581. doi: 10.1161/CIRCULATIONAHA.115.018383. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
