

Loss of Endothelium-Derived Wnt5a Is Associated With Reduced Pericyte Recruitment and Small Vessel Loss in Pulmonary Arterial Hypertension
- PMID: 30586764
- PMCID: PMC6443444
- DOI: 10.1161/CIRCULATIONAHA.118.037642
Loss of Endothelium-Derived Wnt5a Is Associated With Reduced Pericyte Recruitment and Small Vessel Loss in Pulmonary Arterial Hypertension
Abstract
Background: Pulmonary arterial hypertension (PAH) is a life-threatening disorder of the pulmonary circulation associated with loss and impaired regeneration of microvessels. Reduced pericyte coverage of pulmonary microvessels is a pathological feature of PAH and is caused partly by the inability of pericytes to respond to signaling cues from neighboring pulmonary microvascular endothelial cells (PMVECs). We have shown that activation of the Wnt/planar cell polarity pathway is required for pericyte recruitment, but whether production and release of specific Wnt ligands by PMVECs are responsible for Wnt/planar cell polarity activation in pericytes is unknown.
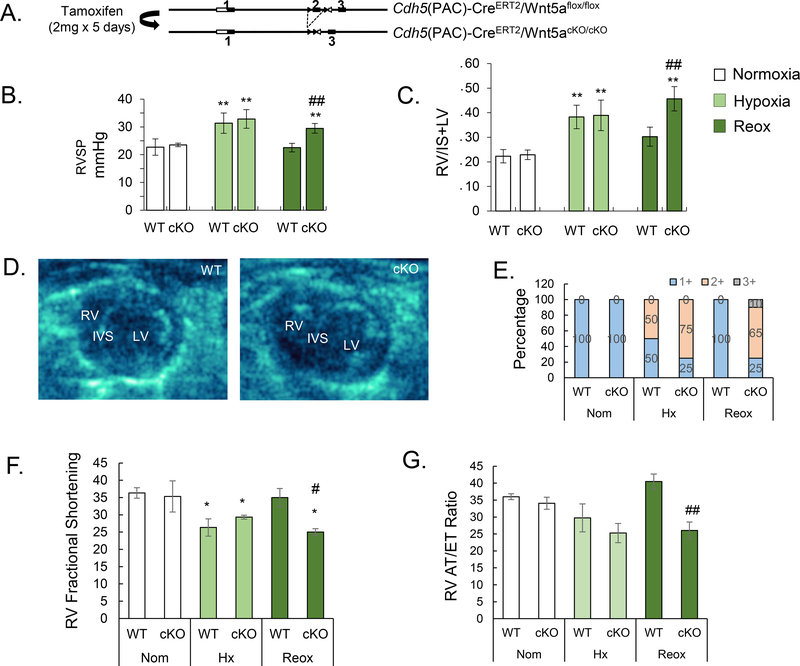
Methods: Isolation of pericytes and PMVECs from healthy donor and PAH lungs was carried out with 3G5 or CD31 antibody-conjugated magnetic beads. Wnt expression profile of PMVECs was documented via quantitative polymerase chain reaction with a Wnt primer library. Exosome purification from PMVEC media was carried out with the ExoTIC device. Hemodynamic profile, right ventricular function, and pulmonary vascular morphometry were obtained in a conditional endothelium-specific Wnt5a knockout ( Wnt5aECKO) mouse model under normoxia, chronic hypoxia, and hypoxia recovery.
Results: Quantification of Wnt ligand expression in healthy PMVECs cocultured with pericytes demonstrated a 35-fold increase in Wnt5a, a known Wnt/planar cell polarity ligand. This Wnt5a spike was not seen in PAH PMVECs, which correlated with an inability to recruit pericytes in Matrigel coculture assays. Exosomes purified from media demonstrated an increase in Wnt5a content when healthy PMVECs were cocultured with pericytes, a finding that was not observed in exosomes of PAH PMVECs. Furthermore, the addition of either recombinant Wnt5a or purified healthy PMVEC exosomes increased pericyte recruitment to PAH PMVECs in coculture studies. Although no differences were noted in normoxia and chronic hypoxia, Wnt5aECKO mice demonstrated persistent pulmonary hypertension and right ventricular failure 4 weeks after recovery from chronic hypoxia, which correlated with significant reduction, muscularization, and decreased pericyte coverage of microvessels.
Conclusions: We identify Wnt5a as a key mediator for the establishment of pulmonary endothelium-pericyte interactions, and its loss could contribute to PAH by reducing the viability of newly formed vessels. We speculate that therapies that mimic or restore Wnt5a production could help prevent loss of small vessels in PAH.
Keywords: Wnt5a; endothelial cells; exosomes; pericytes; pulmonary hypertension.
Figures








References
-
- Ribatti D, Nico B and Crivellato E. The role of pericytes in angiogenesis. Int J Dev Bio. 2011;55:261–268. - PubMed
-
- Yamagishi S and Imaizumi T. Pericyte biology and diseases. Int J Tissue React 2005;27:125–135. - PubMed
-
- Diaz-Flores L, Gutierrez R, Madrid JF, Varela H, Valladares F, Acosta E, Martin-Vasallo P and Diaz-Flores L Jr. Pericytes. Morphofunction, interactions and pathology in a quiescent and activated mesenchymal cell niche. Histol Histopathol. 2009;24:909–969. - PubMed
-
- Kapanci Y, Ribaux C, Chaponnier C and Gabbiani G. Cytoskeletal features of alveolar myofibroblasts and pericytes in normal human and rat lung. J Histochem Cytochem. 1992;40:1955–1963. - PubMed
-
- Teichert-Kuliszewska K, Kutryk MJ, Kuliszewski MA, Karoubi G, Courtman DW, Zucco L, Granton J and Stewart DJ. Bone morphogenetic protein receptor-2 signaling promotes pulmonary arterial endothelial cell survival: implications for loss-of-function mutations in the pathogenesis of pulmonary hypertension. Circ Res. 2006;98:209–217. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
