

Physiological predictors Of peak inspiRatory flow using Observed lung function resultS (POROS): evaluation at discharge among patients hospitalized for a COPD exacerbation
- PMID: 30587952
- PMCID: PMC6296178
- DOI: 10.2147/COPD.S174371
Physiological predictors Of peak inspiRatory flow using Observed lung function resultS (POROS): evaluation at discharge among patients hospitalized for a COPD exacerbation
Abstract
Background: Peak inspiratory flow (PIF) as generated through the resistance of a dry powder inhaler (DPI) device is a critical patient-dependent maneuver impacting the success of DPI medication delivery. Despite its importance, it is not routinely measured in clinical practice. Little is currently known about the relationship, if any, between PIF through DPI devices, routine spirometry and disease outcomes.
Aim: The aim of this study was to identify potential predictors of PIF for different DPIs from spirometric parameters and patient characteristics and explore the association between PIF and follow-up events.
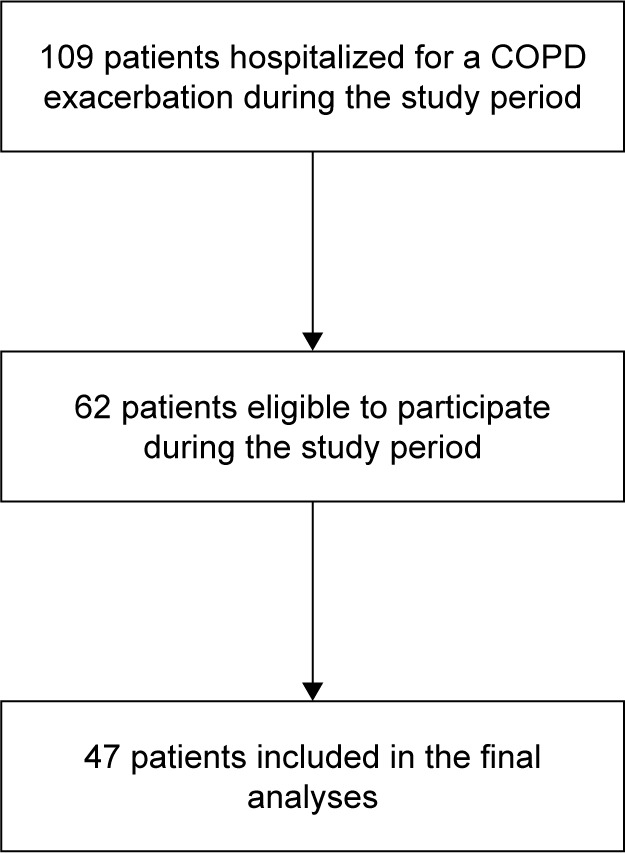
Patients and methods: A retrospective observational study at discharge among patients hospitalized for a COPD exacerbation at Attikon hospital, Athens, Greece. Spirometry was performed using an Easy on-PC™ spirometer. PIF was measured through four DPI resistances using the In-Check™ DIAL. Regression analyses were used to investigate the association between PIF through resistances and spirometric parameters obtained at discharge, comorbidities and demographic parameters.
Results: Forty-seven COPD patients (mean [±SD], age 71 [±9] years, 72% males, 51% current smokers) were included in this study. Overall, 85% and 15% were classified as GOLD (2017) groups D and C, respectively. Most prevalent comorbidities were hypertension (70%) and cardiovascular disease (53%). In the final regression model, higher PIF was significantly associated with the following: higher FEV1 and % predicted peak expiratory flow (PEF) for Turbohaler® (R-squared value 0.374); higher FEV1 and diagnosis of gastroesophageal reflux disease (GERD) for Aerolizer® (R-squared value 0.209) and higher FEV1, younger age and diagnosis of ischemic heart disease (IHD) for Diskus® (R-squared value 0.350). However, R-squared values for all three devices were weak (<0.4).
Conclusion: The study did not provide evidence to support the use of surrogate measurements for PIF through device resistance, which could assist in determining the appropriateness of inhaler device type. Although PIF measurement is feasible in patients at discharge and could be a valuable addition to the standard of care in COPD management, it needs to be measured directly.
Keywords: COPD; dry powder inhaler devices; hospital admission; inhaler technique; resistance; spirometry.
Conflict of interest statement
Disclosure David B Price has board membership with Aerocrine, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Mundipharma, Napp, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Teva Pharmaceuticals; consultancy agreements with Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mylan, Mundipharma, Napp, Novartis, Pfizer, Teva Pharmaceuticals, Theravance; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from Aerocrine, AKL Research and Development Ltd, AstraZeneca, Boehringer Ingelheim, British Lung Foundation, Chiesi, Mylan, Mundipharma, Napp, Novartis, Pfizer, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Teva Pharmaceuticals, Theravance, UK National Health Service, Zentiva (Sanofi Generics); payment for lectures/speaking engagements from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Merck, Mundipharma, Novartis, Pfizer, Regeneron Pharmaceuticals, Sanofi Genzyme, Skyepharma, Teva Pharmaceuticals; payment for manuscript preparation from Mundipharma, Teva Pharmaceuticals; payment for the development of educational materials from Mundipharma, Novartis; payment for travel/accommodation/meeting expenses from Aerocrine, AstraZeneca, Boehringer Ingelheim, Mundipharma, Napp, Novartis, Teva Pharmaceuticals; funding for patient enrolment or completion of research from Chiesi, Novartis, Teva Pharmaceuticals, Zentiva (Sanofi Generics); stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 74% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); and is peer reviewer for grant committees of the Efficacy and Mechanism Evaluation programme, and Health Technology Assessment. David B Price is owner and managing director of Observational and Pragmatic Research Institute Pte Ltd. Vicky Kritikos has received honoraria from AstraZeneca, GlaxoSmithKline and Pfizer. Sinthia Z Bosnic-Anticevich has received honoraria from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Mundipharma and Teva Pharmaceuticals for her contribution to advisory boards/key international expert forum. Victoria Carter, Sen Yang, Antony Hardjojo and Simon Wan Yau Ming are employees of the Observational and Pragmatic Research Institute Pte Ltd, which has conducted paid research in respiratory disease on behalf of the following organizations in the past 5 years: Anaxys, AstraZeneca, Boehringer Ingelheim, British Lung Foundation, Chiesi, Circassia (formerly Aerocrine), Glaxo-SmithKline, Harvey Walsh, Mapi, Morningside Healthcare, Mundipharma, Mylan (formerly Meda), Napp, Novartis, Orion, Plymouth University, Regeneron, Respiratory Effectiveness Group, Roche, Sanofi, Takeda, Teva, University of East Anglia, Zentiva (a Sanofi company). Paul M Dorinsky is an employee of Pearl – a member of the AstraZeneca Group. Claudia Cabrera is an employee of AstraZeneca. Andriana I Papaioannou and Stelios Loukides declare no relevant conflicts of interest. The authors report no other conflicts of interest in this work.
Similar articles
-
Measuring Peak Inspiratory Flow in Patients with Chronic Obstructive Pulmonary Disease.Int J Chron Obstruct Pulmon Dis. 2022 Jan 6;17:79-92. doi: 10.2147/COPD.S319511. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 35023914 Free PMC article. Review.
-
Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD.Int J Chron Obstruct Pulmon Dis. 2019 Mar 1;14:585-595. doi: 10.2147/COPD.S195438. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 30880948 Free PMC article.
-
Changes in Peak Inspiratory Flow After Acute Bronchodilation: An Observational Study of Patients with Stable Chronic Obstructive Pulmonary Disease.J Aerosol Med Pulm Drug Deliv. 2024 Aug;37(4):171-179. doi: 10.1089/jamp.2023.0045. Epub 2024 May 29. J Aerosol Med Pulm Drug Deliv. 2024. PMID: 38814000
-
[The variability of peak inspiratory flow (PIF) on valves imitating dry powder inhalers resistance during asthma and COPD exacerbations].Pneumonol Alergol Pol. 2007;75(4):324-30. Pneumonol Alergol Pol. 2007. PMID: 18080981 Polish.
-
Relationship between Peak Inspiratory Flow and Patient and Disease Characteristics in Individuals with COPD-A Systematic Scoping Review.Biomedicines. 2022 Feb 16;10(2):458. doi: 10.3390/biomedicines10020458. Biomedicines. 2022. PMID: 35203667 Free PMC article.
Cited by
-
Measuring Peak Inspiratory Flow in Patients with Chronic Obstructive Pulmonary Disease.Int J Chron Obstruct Pulmon Dis. 2022 Jan 6;17:79-92. doi: 10.2147/COPD.S319511. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 35023914 Free PMC article. Review.
-
Impact of PIF, Inhalation Technique and Medication Adherence on Health Status and Exacerbations in COPD: Protocol of a Real-World Observational Study (PIFotal COPD Study).Pulm Ther. 2021 Dec;7(2):591-606. doi: 10.1007/s41030-021-00172-7. Epub 2021 Sep 17. Pulm Ther. 2021. PMID: 34533772 Free PMC article.
-
Clinical Burden of Chronic Obstructive Pulmonary Disease in Patients with Suboptimal Peak Inspiratory Flow.Can Respir J. 2024 Mar 22;2024:8034923. doi: 10.1155/2024/8034923. eCollection 2024. Can Respir J. 2024. PMID: 38560416 Free PMC article.
-
TRONARTO: A Randomized, Placebo-Controlled Study of Tiotropium/Olodaterol Delivered via Soft Mist Inhaler in COPD Patients Stratified by Peak Inspiratory Flow.Int J Chron Obstruct Pulmon Dis. 2021 Aug 28;16:2455-2465. doi: 10.2147/COPD.S324467. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 34511891 Free PMC article. Clinical Trial.
-
Suboptimal Peak Inspiratory Flow in Patients Hospitalized for COPD Exacerbation: Prevalence and Predictive Factors.J Aerosol Med Pulm Drug Deliv. 2024 Oct;37(5):225-231. doi: 10.1089/jamp.2024.0002. Epub 2024 Jun 19. J Aerosol Med Pulm Drug Deliv. 2024. PMID: 39388689
References
-
- Global Initiative for Chronic Obstructive Lung Disease [homepage on the Internet] From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2018. [Accessed January 2, 2018]. Report. Available from: www.goldcopd.org.
-
- Barnes PJ. Immunology of asthma and chronic obstructive pulmonary disease. Nat Rev Immunol. 2008;8(3):183–192. - PubMed
-
- Choudhury G, Rabinovich R, Macnee W. Comorbidities and systemic effects of chronic obstructive pulmonary disease. Clin Chest Med. 2014;35(1):101–130. - PubMed
-
- Corlateanu A, Covantev S, Mathioudakis AG, Botnaru V, Siafakas N. Prevalence and burden of comorbidities in Chronic Obstructive Pulmonary Disease. Respir Investig. 2016;54(6):387–396. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
