

The cost impact to Medicare of shifting treatment of worsening heart failure from inpatient to outpatient management settings
- PMID: 30588047
- PMCID: PMC6298883
- DOI: 10.2147/CEOR.S184048
The cost impact to Medicare of shifting treatment of worsening heart failure from inpatient to outpatient management settings
Abstract
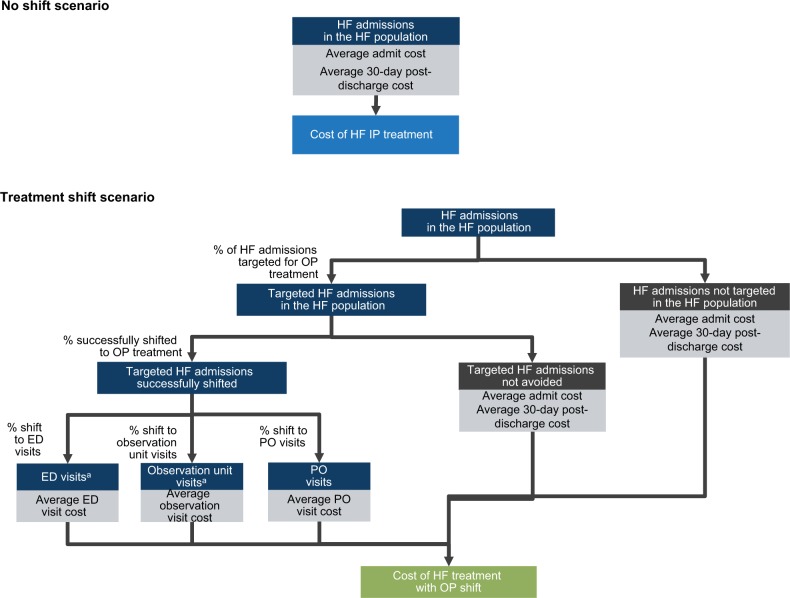
Purpose: The aim of this study was to quantify the potential cost savings to Medicare of shifting the site of treatment for worsening heart failure (HF) from inpatient to outpatient (OP) settings for a subset of worsening HF episodes among the Medicare fee-for-service (FFS) population.
Materials and methods: A cross-sectional analysis of a random 5% sample of 2014 FFS Medicare beneficiaries was conducted. Incidence and cost of worsening HF episodes in both inpatient and OP settings were identified. These results were used to calculate cost savings associated with shifting a proportion of worsening HF episodes from the inpatient to OP settings.
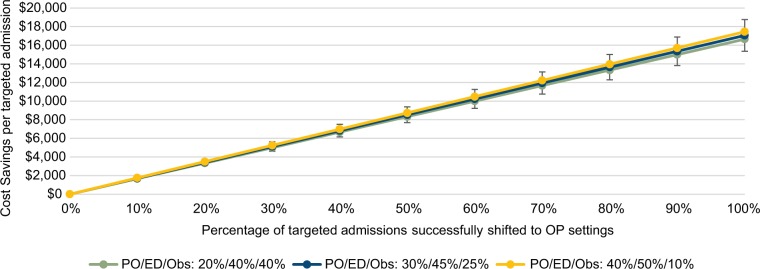
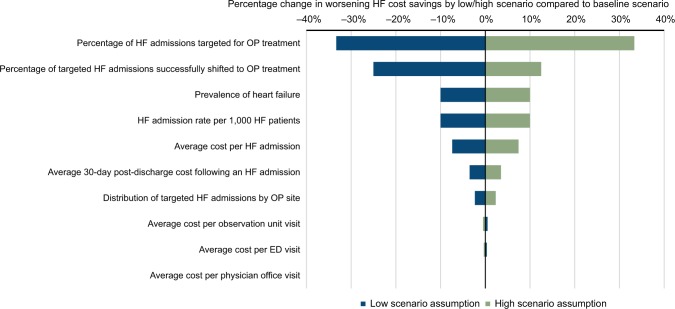
Results: A total of 151,908 HF beneficiaries were identified. The estimated annual cost for the treatment of worsening HF across both inpatient and OP settings ranged from US$9.3 billion to US$17.0 billion or 2.4%-4.3% of total Medicare FFS spend. The cost saving associated with shifting worsening HF treatment from inpatient hospital setting to OP settings was US$667.5 million or 0.17% of total Medicare spend when 10% of HF admissions were targeted and 60% of targeted HF admissions were successfully shifted. The cost savings increased to US$2.098 billion or 0.53% of total Medicare spend when 20% of HF admissions were targeted and 90% of targeted HF admissions were successfully shifted.
Conclusion: Treatment options that can shift costly hospital admissions for worsening HF treatment to less expensive OP settings potentially lead to significant cost savings to Medicare. Pursuit of OP therapy options for treating worsening HF might be considered a viable alternative.
Keywords: administrative claims data; cost impact analysis; health care resource utilization; heart failure management; hospital admission burden.
Conflict of interest statement
Disclosure Kathryn Fitch is a Principal of the New York Health Practice of Milliman, Inc. Jocelyn Lau and Tyler Engel are employees of Milliman, Inc. Kathryn Fitch received consulting fees from scPharmaceuticals, Inc. to conduct this study. Dr. William S Weintraub is the Director of Outcomes Research at MedStar Washington Hospital Center. Drs. Joseph J Medicis and John F Mohr are employees and stock holders of scPharmaceuticals. Dr. Joseph J Medicis is Senior Director, Medical Affairs, at scPharmaceuticals, Inc. and Dr. John F Mohr is Vice President, Clinical Development and Medical Affairs at scPharmaceuticals, Inc. The authors report no other conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
