

The comorbidities of dysmenorrhea: a clinical survey comparing symptom profile in women with and without endometriosis
- PMID: 30588070
- PMCID: PMC6300370
- DOI: 10.2147/JPR.S179409
The comorbidities of dysmenorrhea: a clinical survey comparing symptom profile in women with and without endometriosis
Abstract
Purpose: Dysmenorrhea is a common disorder that substantially disrupts the lives of young women. The frequency of 14 associated symptoms both within and outside the pelvis was determined.
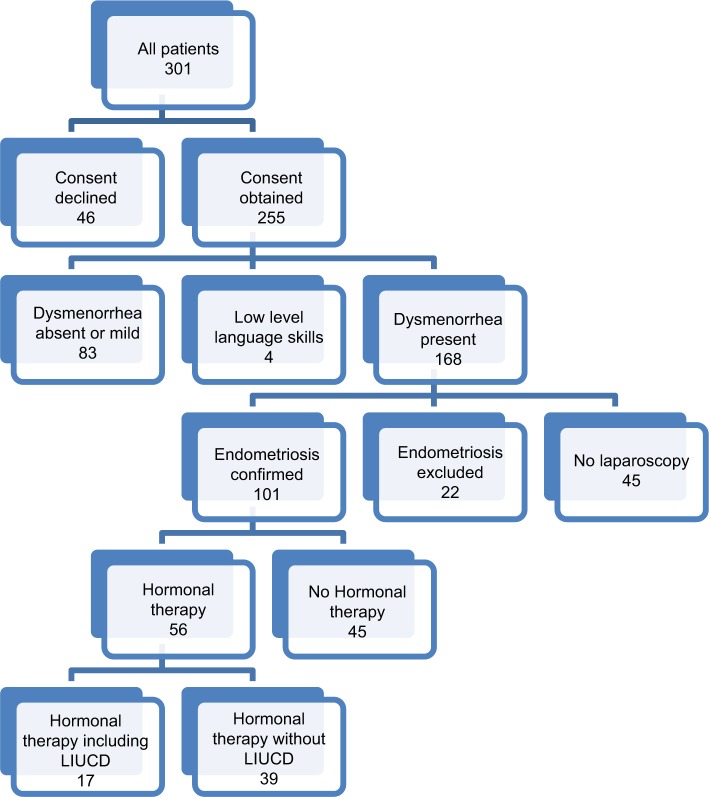
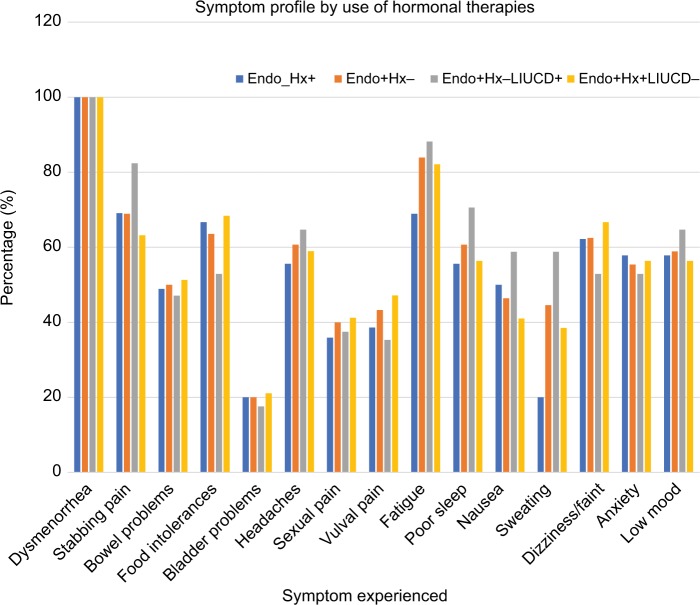
Patients and methods: Symptom questionnaires were completed by 168 women with dysmenorrhea, allocated to three groups based on their diagnostic status for endometriosis confirmed (Endo+), endometriosis excluded (Endo-), or endometriosis diagnosis unknown (No Lap). Those with endometriosis confirmed were further divided into current users (Endo+ Hx+) and non-users of hormonal treatments (Endo+ Hx-). Users of hormonal treatments were further divided into users (Endo+ Hx+ LIUCD+) and non-users (Endo+ Hx+ LIUCD-) of a levonorgestrel-releasing intra-uterine contraceptive device (LIUCD). The frequency and number of symptoms within groups and the effect of previous distressing sexual events were sought.
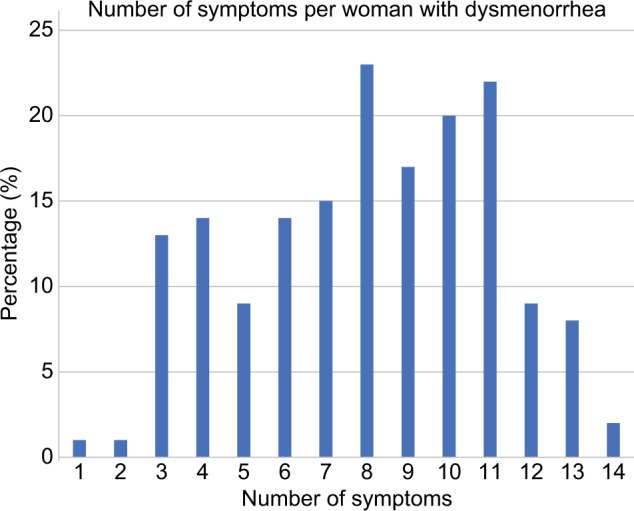
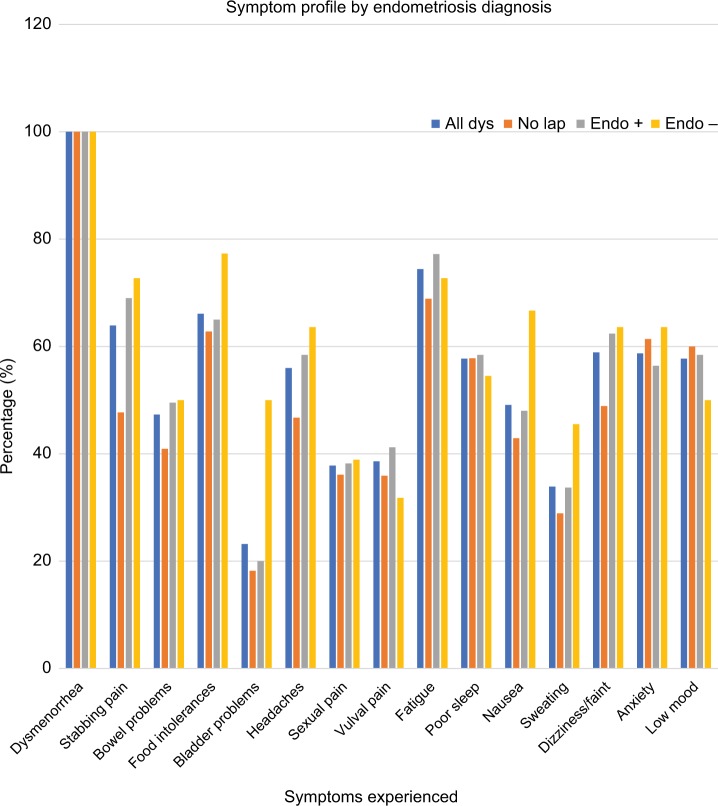
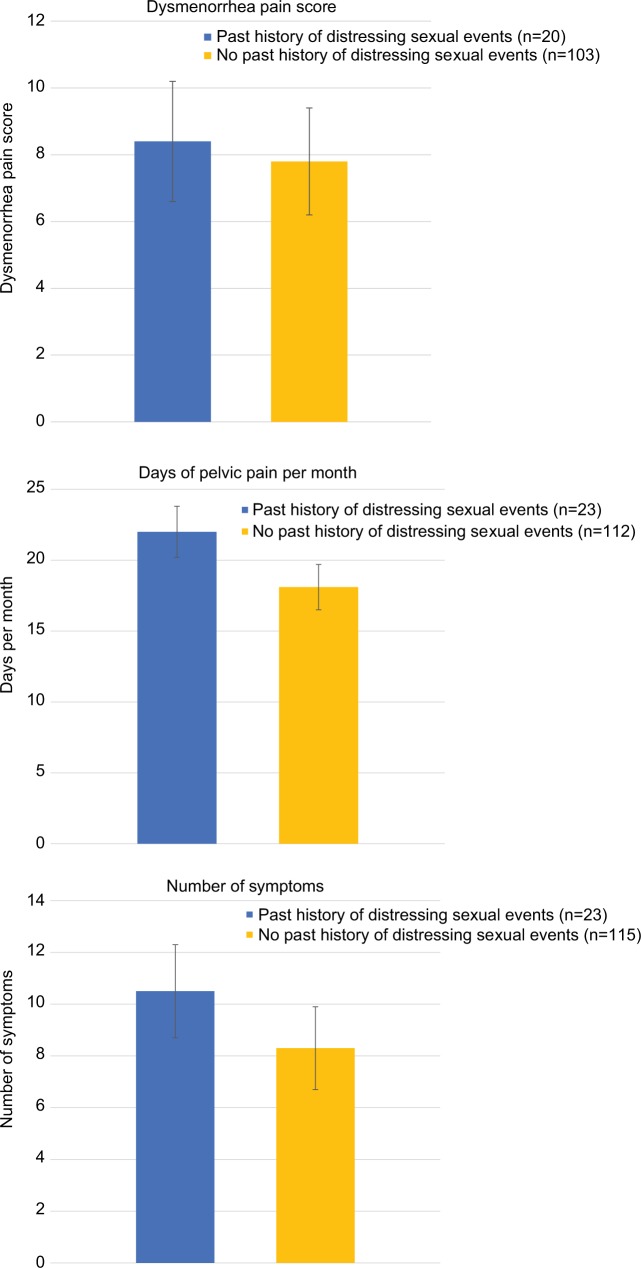
Results: Women with and without endometriosis lesions had similar symptom profiles, with a mean of 8.5 symptoms per woman. Only 0.6% of women reported dysmenorrhea alone. The presence of stabbing pelvic pains was associated with more severe dysmenorrhea (P=0.006), more days per month of dysmenorrhea (P=0.003), more days per month of pelvic pain (P=0.016), and a diagnosis of migraine (P=0.054). The symptom profiles of the Endo+ Hx+ and Endo+ Hx- groups were similar. A history of distressing sexual events was associated with an increased number of pain symptoms (P=0.003).
Conclusion: Additional symptoms are common in women with dysmenorrhea, and do not correlate with the presence or absence of endometriosis lesions. Our study supports the role of central sensitization in the pain of dysmenorrhea. The presence of stabbing pelvic pains was associated with increased severity of dysmenorrhea, days per month of dysmenorrhea, days per month of pelvic pain, and a diagnosis of migraine headache. A past history of distressing sexual events is associated with an increased number of pain symptoms.
Keywords: bladder pain syndrome; chronic pain; dysmenorrhea; endometriosis; headache; levonorgestrel-releasing intra-uterine device; pelvic pain; stabbing pain.
Conflict of interest statement
Disclosure SFE received royalties from book authorship, has received payment from Pfizer and Bayer for educational presentations, and is involved in the development of novel treatments for pelvic pain. PER is a shareholder in Havah Therapeutics and iXBiopharma, director and shareholder of Lipotek, consultant to Bionomics and Novartis, and has received payment for educational presentations from Novartis and Sequirus. The other authors report no conflicts of interest in this work.
Figures
References
-
- Ju H, Jones M, Mishra G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev. 2014;36:104–113. - PubMed
-
- Parker MA, Sneddon AE, Arbon P. The menstrual disorder of teenagers (MDOT) study: determining typical menstrual patterns and menstrual disturbance in a large population-based study of Australian teenagers. BJOG. 2010;117(2):185–192. - PubMed
-
- Hardi G, Evans S, Craigie M. A possible link between dysmenorrhoea and the development of chronic pelvic pain. Aust N Z J Obstet Gynaecol. 2014;54(6):593–596. - PubMed
-
- Janssen EB, Rijkers AC, Hoppenbrouwers K, Meuleman C, D’Hooghe TM. Prevalence of endometriosis diagnosed by laparoscopy in adolescents with dysmenorrhea or chronic pelvic pain: a systematic review. Hum Reprod Update. 2013;19(5):570–582. - PubMed
-
- Jarrell J, Arendt-Nielsen L. Allodynia and Dysmenorrhea. JOGC. 2016;38(3):270–274. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
