

Identifying Risk and Management of Acute Haemodynamic Decompensation During Catheter Ablation of Ventricular Tachycardia
- PMID: 30588317
- PMCID: PMC6304792
- DOI: 10.15420/aer.2018.36.3
Identifying Risk and Management of Acute Haemodynamic Decompensation During Catheter Ablation of Ventricular Tachycardia
Abstract
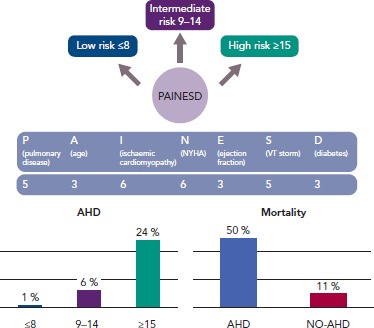
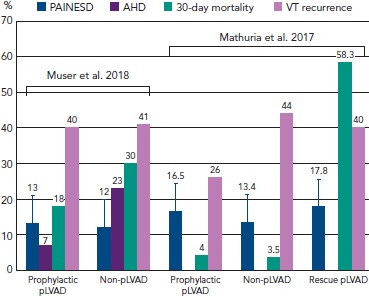
Radiofrequency catheter ablation (CA) has an established role in the management of patients with structural heart disease presenting with recurrent ventricular tachycardia (VT). Due to the complex underlying substrate, high burden of comorbidities and concomitant heart failure (HF) status, these patients may be at higher risk of periprocedural complications. The prolonged low-output state related to VT induction and mapping, as well as the fluid overload due to irrigated CA and the use of general anaesthesia, may decompensate the HF status, leading to multiple-organ failure and increase in early post-procedural mortality. Proper identification of patients at high risk of periprocedural acute haemodynamic decompensation (AHD) has important implications in terms of procedural planning (i.e. prophylactic use of mechanical assistance devices) and pre-procedural management in order to optimise the HF status. In the present manuscript we focus on the clinical predictors of AHD and the strategies to improve pre-procedural risk stratification, as well as the evidence supporting the use of haemodynamic support during CA procedures.
Keywords: Haemodynamic decompensation; catheter ablation; mechanical haemodynamic support; ventricular tachycardia.
Conflict of interest statement
Disclosure: The authors have no conflicts of interest to declare.
Figures
References
-
- Santangeli P, Muser D, Maeda S et al. Comparative effectiveness of antiarrhythmic drugs and catheter ablation for the prevention of recurrent ventricular tachycardia in patients with implantable cardioverter-defibrillators: a systematic review and meta-analysis of randomized controlled trials. Heart Rhythm. 2016;13:1552–9. doi: 10.1016/j.hrthm.2016.03.004. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
