

Arthroscopic All-Inside Anterior Talofibular Ligament Repair Through a Three-Portal and No-Ankle-Distraction Technique
- PMID: 30588370
- PMCID: PMC6292720
- DOI: 10.2106/JBJS.ST.18.00026
Arthroscopic All-Inside Anterior Talofibular Ligament Repair Through a Three-Portal and No-Ankle-Distraction Technique
Abstract
Background: Ankle instability is a common consequence of ankle sprains. Injury of the anterior talofibular ligament (ATFL) is the most common cause of ankle instability1. Arthroscopic treatment of ankle instability is an emerging field attracting increased interest among surgeons2-10. The arthroscopic all-inside ATFL repair allows the surgeon to explore the ankle joint, treat concomitant pathology when encountered, and reattach the injured ATFL to its fibular anatomical location. The aim of this article is to describe the arthroscopic all-inside ATFL repair through a 3-portal no-ankle-distraction technique.
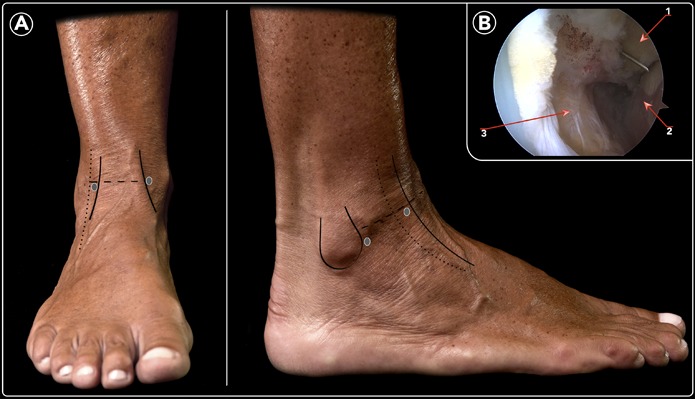
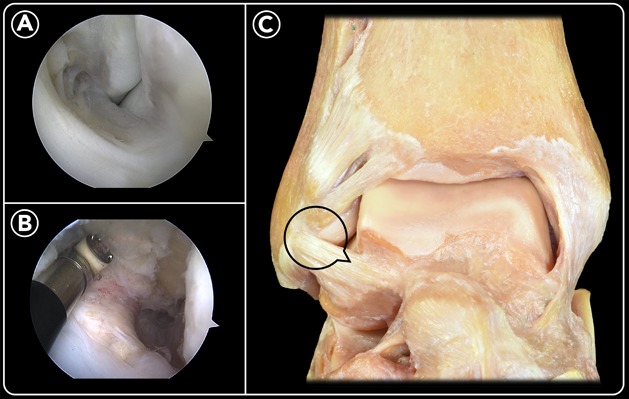
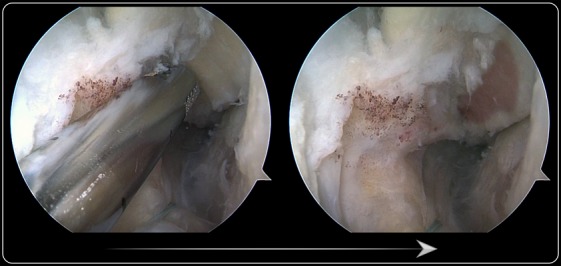
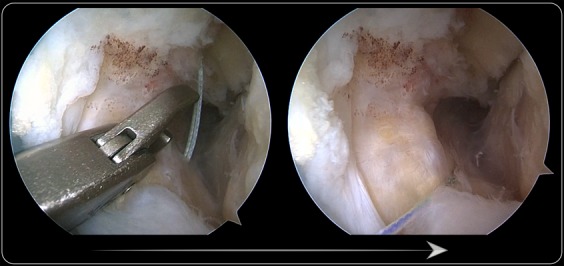
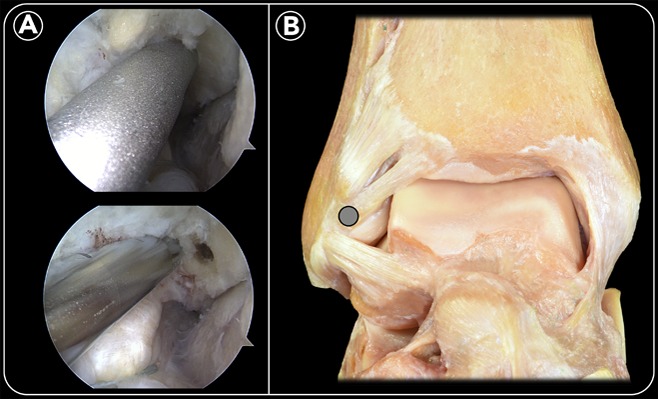
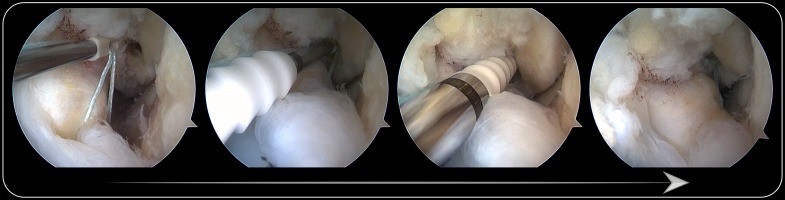
Description: After patient positioning, anteromedial and anterolateral portals are created. An accessory anterolateral portal is created just anterior to the fibula and about 1 cm proximal to the tip of the lateral malleolus. The arthroscope is introduced through the anteromedial portal, and the instruments are introduced through the anterolateral portal. Recognition of the ligament and evaluation of the ligament tear with a probe are required. The footprint for the fibular attachment of the ATFL is debrided. The ligament is penetrated with a suture passer. A nitinol loop is pushed and then is pulled out through the accessory portal. The nitinol wire is replaced by a double high-resistance suture. The limbs of the suture located in the accessory portal are passed through the anterolateral portal. Next, one or both limbs of the suture are passed through the loop suture. Pulling of the suture limbs introduces the loop into the joint and the ligament is grasped by the suture. The tunnel for the anchor is drilled. The knotless anchor is loaded with the suture, and the anchor and suture are introduced with the ankle in dorsiflexion and valgus. Postoperatively, the ankle is immobilized with a removable walking boot for 4 weeks. Once use of the walking boot is discontinued, physical therapy is started.
Alternatives: Nonoperative treatment with physiotherapy or sports restriction can be an alternative for patients with surgical contraindications or as a first step of treatment. Open techniques (repair or reconstruction) or other arthroscopic-assisted techniques (arthroscopic introduction of anchors and percutaneous passage of sutures, or arthroscopic-assisted reconstruction) are possible surgical alternatives to the described technique to treat ankle instability.
Rationale: The described technique has the advantage of being done with a minimally invasive approach and providing an anatomical repair of the ligament. Concomitant intra-articular pathology can be addressed during the procedure through the same arthroscopic approaches. Early rehabilitation and the lack of intra-articular knots are additional benefits of the technique.
Figures


Similar articles
-
Clinical Outcomes for Arthroscopic Anterior Talofibular Ligament Repair After Suture Anchor Insertion Through the Anterolateral Portal vs the Lateral Accessory Portal.Foot Ankle Int. 2024 Oct;45(10):1093-1101. doi: 10.1177/10711007241265354. Epub 2024 Jul 30. Foot Ankle Int. 2024. PMID: 39080925
-
Arthroscopic all-inside anterior talo-fibular ligament repair with suture augmentation gives excellent results in case of poor ligament tissue remnant quality.Knee Surg Sports Traumatol Arthrosc. 2020 Jan;28(1):100-107. doi: 10.1007/s00167-018-5117-x. Epub 2018 Aug 20. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 30128684
-
Arthroscopic all-inside ATFL and CFL repair is feasible and provides excellent results in patients with chronic ankle instability.Knee Surg Sports Traumatol Arthrosc. 2020 Jan;28(1):116-123. doi: 10.1007/s00167-019-05676-z. Epub 2019 Aug 20. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31432243
-
[Arthroscopic repair of chronic lateral ankle instability].Oper Orthop Traumatol. 2019 Jun;31(3):201-210. doi: 10.1007/s00064-019-0595-7. Epub 2019 Mar 27. Oper Orthop Traumatol. 2019. PMID: 30918997 Review. German.
-
[Lateral ankle ligament bracing].Oper Orthop Traumatol. 2019 Jun;31(3):191-200. doi: 10.1007/s00064-019-0603-y. Epub 2019 May 16. Oper Orthop Traumatol. 2019. PMID: 31098649 Review. German.
Cited by
-
The lateral ankle ligaments are interconnected: the medial connecting fibres between the anterior talofibular, calcaneofibular and posterior talofibular ligaments.Knee Surg Sports Traumatol Arthrosc. 2020 Jan;28(1):34-39. doi: 10.1007/s00167-019-05794-8. Epub 2019 Nov 22. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31754730
-
Arthroscopic anterior talofibular ligament repair with Internal Brace and lasso-loop technique for chronic ankle lateral instability.Int Orthop. 2022 Dec;46(12):2821-2828. doi: 10.1007/s00264-022-05541-8. Epub 2022 Sep 7. Int Orthop. 2022. PMID: 36069956
-
The arthroscopic all-inside ankle lateral collateral ligament repair is a safe and reproducible technique.Knee Surg Sports Traumatol Arthrosc. 2020 Jan;28(1):63-69. doi: 10.1007/s00167-019-05427-0. Epub 2019 Mar 4. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 30830298
-
The lowest point of fibula (LPF) could be used as a reliable bony landmark for arthroscopic anchor placement of lateral ankle ligaments ----compared with open Broström procedure.BMC Musculoskelet Disord. 2023 Sep 26;24(1):759. doi: 10.1186/s12891-023-06876-y. BMC Musculoskelet Disord. 2023. PMID: 37749543 Free PMC article.
-
All-Inside Arthroscopic Anatomic Anterior Talofibular Ligament Repair for Anterolateral Ankle Instability Using a Knotless Suture Anchor, Allowing for Tension Adjustment.Arthrosc Tech. 2021 Feb 22;10(3):e925-e929. doi: 10.1016/j.eats.2020.11.013. eCollection 2021 Mar. Arthrosc Tech. 2021. PMID: 33738234 Free PMC article.
References
-
- Broström L. Sprained ankles. VI. Surgical treatment of “chronic” ligament ruptures. Acta Chir Scand. 1966. November;132(5):551-65. - PubMed
-
- Corte-Real NM, Moreira RM. Arthroscopic repair of chronic lateral ankle instability. Foot Ankle Int. 2009. March;30(3):213-7. - PubMed
-
- Kim ES, Lee KT, Park JS, Lee YK. Arthroscopic anterior talofibular ligament repair for chronic ankle instability with a suture anchor technique. Orthopedics. 2011. April 11;34(4):1-5. - PubMed
-
- Acevedo JI, Mangone PG. Arthroscopic lateral ankle ligament reconstruction. Tech Foot Ankle Surg. 2011. September;10(3):111-6.
-
- Nery C, Raduan F, Del Buono A, Asaumi ID, Cohen M, Maffulli N. Arthroscopic-assisted Broström-Gould for chronic ankle instability: a long-term follow-up. Am J Sports Med. 2011. November;39(11):2381-8. Epub 2011 Jul 29. - PubMed
LinkOut - more resources
Full Text Sources