

Comparison of bilateral/unilateral lateral rectus recession and unilateral recession-resection for intermittent exotropia: a Meta-analysis
- PMID: 30588434
- PMCID: PMC6288523
- DOI: 10.18240/ijo.2018.12.18
Comparison of bilateral/unilateral lateral rectus recession and unilateral recession-resection for intermittent exotropia: a Meta-analysis
Abstract
Aim: To compare the effectiveness of unilateral recession-resection (R&R) and bilateral/unilateral recession (BLR/ULR) for treatment of basic type of intermittent exotropia [IX(T)].
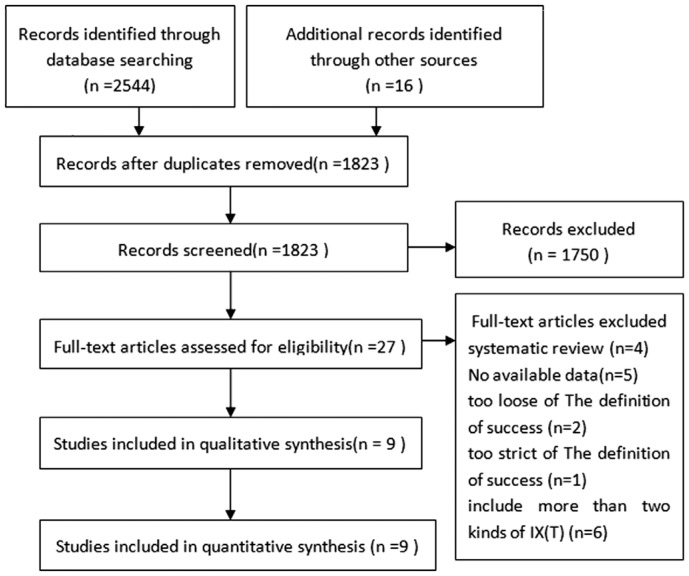
Methods: A comprehensive literature search was performed using PubMed, EMBASE, and the Cochrane Library, to identify randomized controlled trials and comparative studies regarding the effectiveness of R&R and BLR/ULR for IX(T). Based on which, a Meta-analysis was then performed in terms of long-term success rate, overcorrection rate, and recurrence rate.
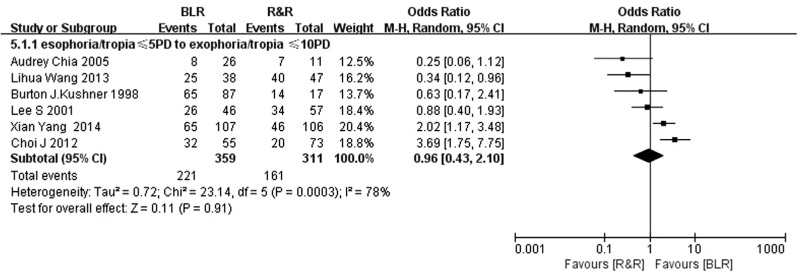
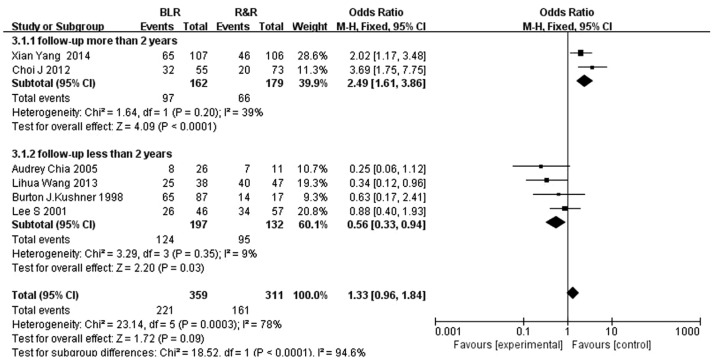
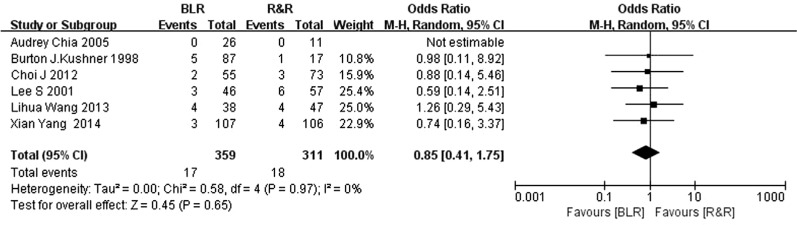
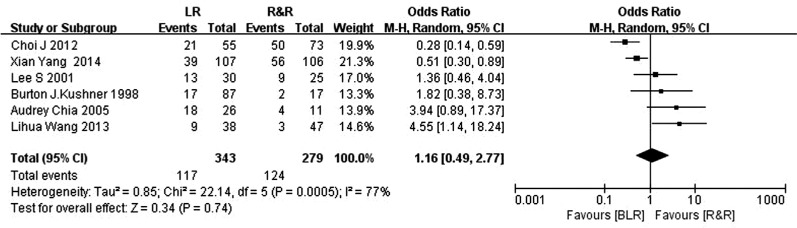
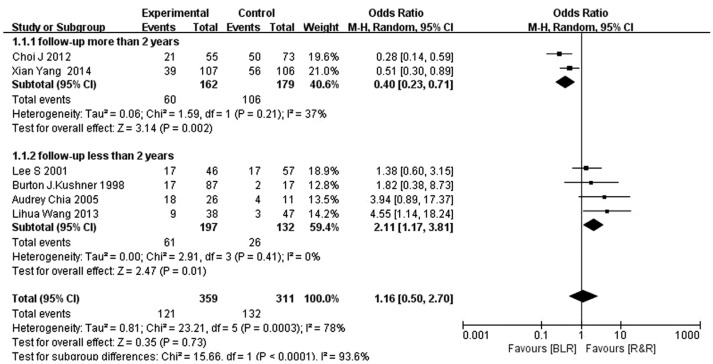
Results: Nine studies in total satisfy the specified eligibility criteria. BLR is at disadvantage to R&R at a short-term follow-up [<2y, OR 0.56 (0.33-0.94) for success rate; OR 2.11 (1.17, 3.81) for undercorrection rate]. However, BLR achieved a higher success rate [OR 2.49 (1.61, 3.86)] and a lower undercorrection rate [OR 0.40 (0.23, 0.71)], compared to that of R&R at a long-term follow-up (>2y). There is no significant difference was found in overcorrection rate, regardless of the length of follow-up time [OR 0.85 (0.41, 1.75)]. In the treatment for small-angle IX(T), the final outcome was significantly different between the groups, demonstrating a more successful alignment [OR 0.37 (0.18, 0.74)] and a lower undercorrection [OR 3.50 (1.28, 7.26)] in the R&R group than in the ULR group. While for moderate-angle IX(T) (20 PD-25 PD), the effectiveness of R&R and ULR is quite equivalent with similar success rate [OR 1.08 (0.65, 1.79)] and undercorrection rate [OR 0.89 (0.54, 1.48)].
Conclusion: As regard to the effect of BLR and R&R, R&R shows an advantage over BLR at short term. But, BLR is more effective in the long term for the basic type IX(T) in children. R&R surgery should be a better choice for the treatment of small-angle IX(T) of ≤20 PD than ULR. However, both of ULR and R&R are recommended for moderate-angle IX(T) from 20 PD to 25 PD.
Keywords: intermittent exotropia; moderate-angle exotropia; recess-resect; unilateral lateral rectus recession.
Figures
Similar articles
-
Comparison of Long-term Surgical Outcomes Between Unilateral Recession and Unilateral Recession-Resection in Small-Angle Exotropia.Am J Ophthalmol. 2016 Jun;166:141-148. doi: 10.1016/j.ajo.2016.03.047. Epub 2016 Apr 8. Am J Ophthalmol. 2016. PMID: 27066724
-
The long-term survival analysis of bilateral lateral rectus recession versus unilateral recession-resection for intermittent exotropia.Am J Ophthalmol. 2012 Feb;153(2):343-351.e1. doi: 10.1016/j.ajo.2011.06.024. Epub 2011 Oct 6. Am J Ophthalmol. 2012. PMID: 21982103
-
Comparison of bilateral lateral rectus recession and unilateral recession resection for basic type intermittent exotropia in children.Br J Ophthalmol. 2013 Jul;97(7):870-3. doi: 10.1136/bjophthalmol-2013-303167. Epub 2013 May 4. Br J Ophthalmol. 2013. PMID: 23645821
-
Bilateral lateral rectus recession versus unilateral recession resection for basic intermittent exotropia: a meta-analysis.Graefes Arch Clin Exp Ophthalmol. 2018 Mar;256(3):451-458. doi: 10.1007/s00417-018-3912-1. Epub 2018 Jan 24. Graefes Arch Clin Exp Ophthalmol. 2018. PMID: 29368040 Review.
-
Efficacy of bilateral lateral rectus recession versus unilateral recession and resection for basic-type intermittent exotropia: a meta-analysis.Acta Ophthalmol. 2021 Nov;99(7):e984-e990. doi: 10.1111/aos.14726. Epub 2021 Feb 11. Acta Ophthalmol. 2021. PMID: 33576184
Cited by
-
How to Better Treat Patients with Intermittent Exotropia: A Review of Surgical Treatment of Intermittent Exotropia.Korean J Ophthalmol. 2022 Dec;36(6):550-564. doi: 10.3341/kjo.2022.0043. Epub 2022 Oct 11. Korean J Ophthalmol. 2022. PMID: 36220643 Free PMC article. Review.
-
Analysis of the Changes and Possible Reasons in Aberrations before and after Surgery in Patients with Concomitant Exotropia.Comput Intell Neurosci. 2022 Sep 5;2022:5207553. doi: 10.1155/2022/5207553. eCollection 2022. Comput Intell Neurosci. 2022. PMID: 36105630 Free PMC article.
References
-
- Nusz KJ, Mohney BG, Diehl NN. The course of intermittent exotropia in a population-based cohort. Ophthalmology. 2006;113(7):1154–1158. - PubMed
-
- Yuksel D, Spiritus M, Vandelannoitte S. Symmetric or asymmetric surgery for basic intermittent exotropia. Bull Soc Belge Ophtalmol. 1998;268:195–199. - PubMed
-
- Burian HM. Exodeviations: their classification, diagnosis and treatment. Am J Ophthalmol. 1966;62(6):1161–1166. - PubMed
-
- Kim SH, Choi YJ. Effects of unilateral lateral rectus recession according to the tendon width in intermittent exotropia. Eye (Lond) 2006;20(7):785–788. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials