

Hemodialysis vascular access and subsequent transplantation: a report from the ESPN/ERA-EDTA Registry
- PMID: 30588548
- PMCID: PMC6394682
- DOI: 10.1007/s00467-018-4129-6
Hemodialysis vascular access and subsequent transplantation: a report from the ESPN/ERA-EDTA Registry
Abstract
Background: Current guidelines advocate use of arteriovenous fistula (AVF) over central venous catheter (CVC) for children starting hemodialysis (HD). European data on current practice, determinants of access choice and switches, patient survival, and access to transplantation are limited.
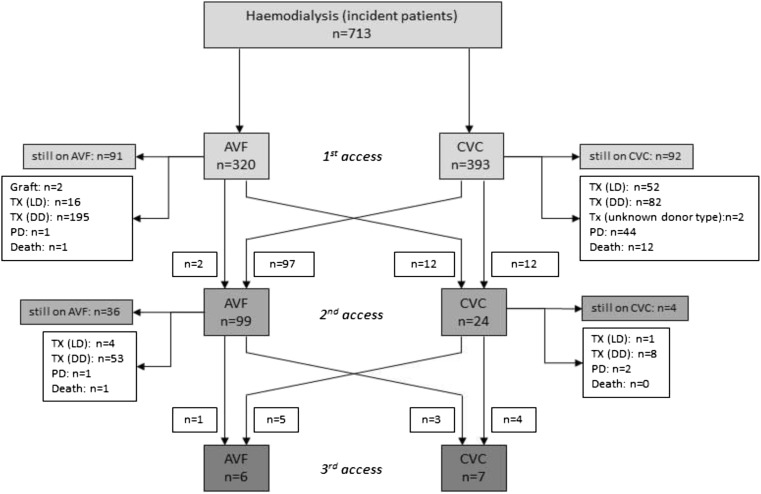
Methods: We included incident patients from 18 European countries who started HD from 2000 to 2013 for whom vascular access type was reported to the ESPN/ERA-EDTA Registry. Data were evaluated using descriptive statistics, logistic and Cox regression models, and cumulative incidence competing risk analysis.
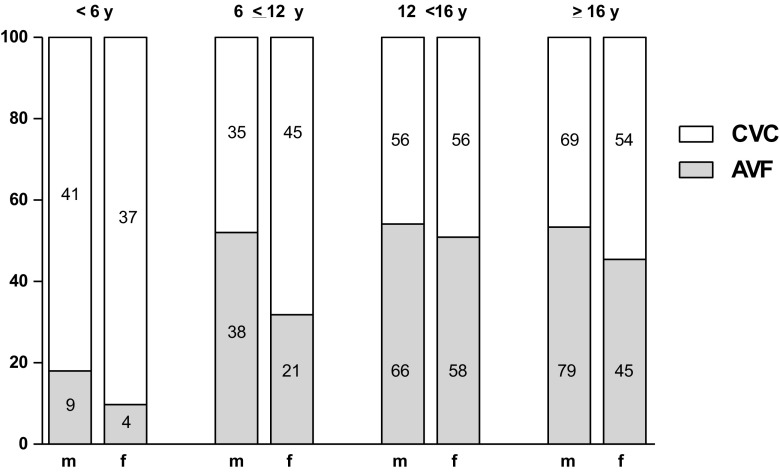
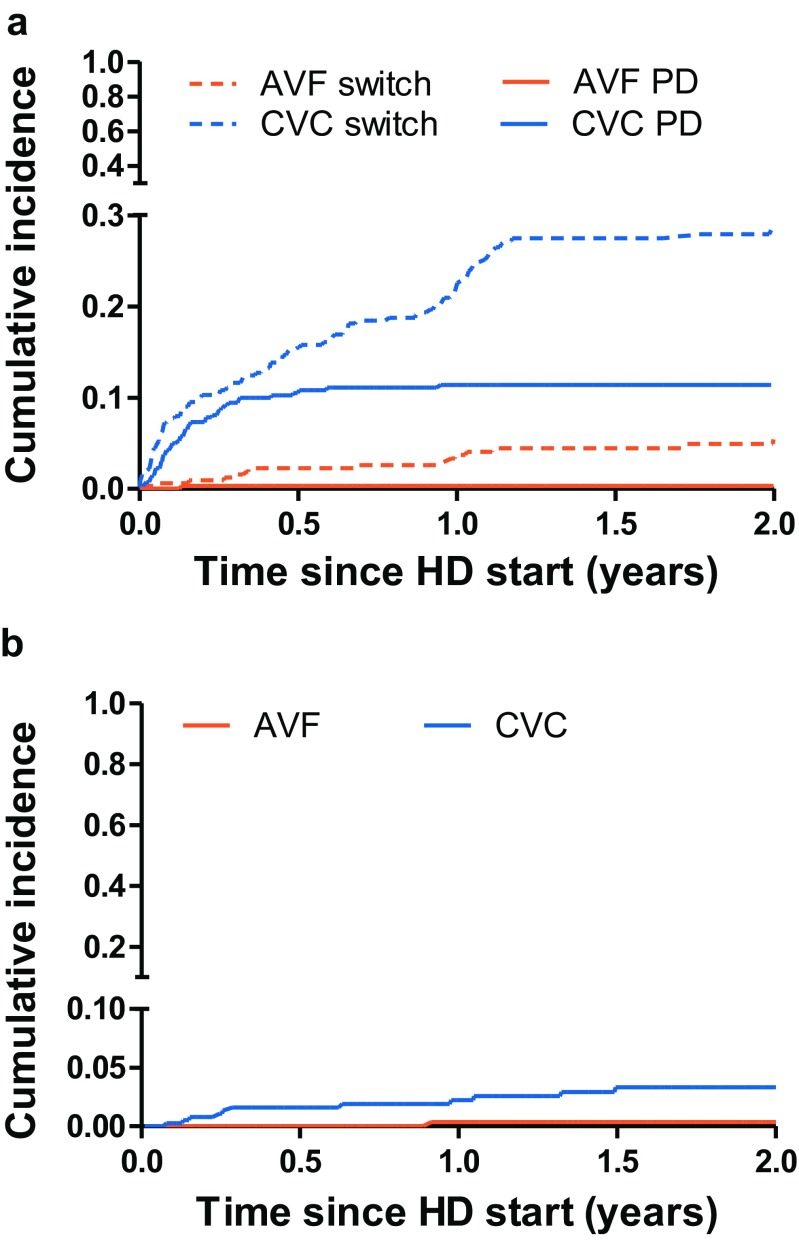
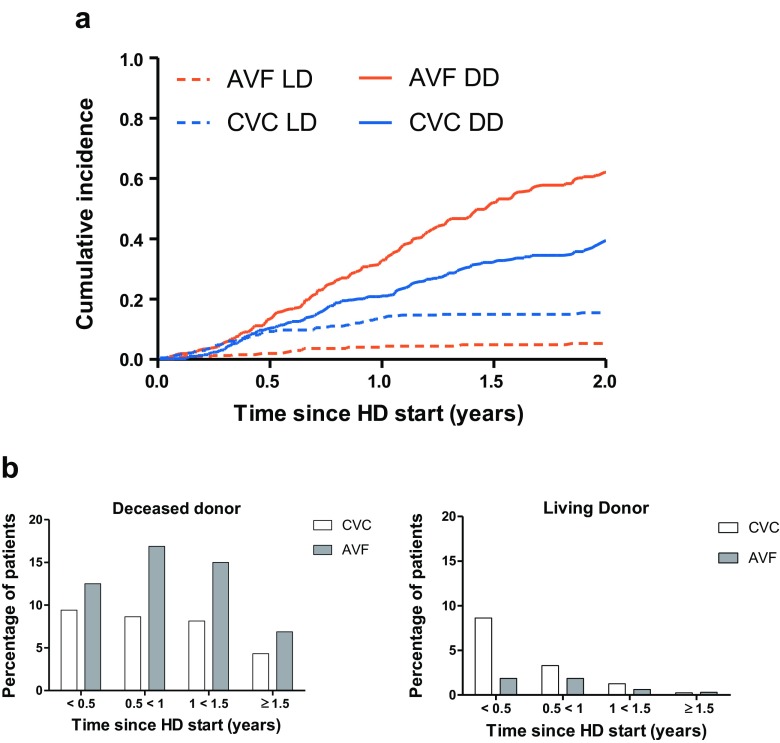
Results: Three hundred ninety-three (55.1%) of 713 children started HD with a CVC and were more often females, younger, had more often an unknown diagnosis, glomerulonephritis, or vasculitis, and lower hemoglobin and height-SDS at HD initiation. AVF patients were 91% less likely to switch to a second access, and two-year patient survival was 99.6% (CVC, 97.2%). Children who started with an AVF were less likely to receive a living donor transplant (adjusted HR, 0.30; 95% CI, 0.16-0.54) and more likely to receive a deceased donor transplant (adjusted HR, 1.50; 95% CI, 1.17-1.93), even after excluding patients who died or were transplanted in the first 6 months.
Conclusions: CVC remains the most frequent type of vascular access in European children commencing HD. Our results suggest that the choice for CVC is influenced by the time of referral, rapid onset of end-stage renal disease, young age, and an expected short time to transplantation. The role of vascular access type on the pattern between living and deceased donation in subsequent transplantation requires further study.
Keywords: Access to transplantation; Arteriovenous fistula; Central venous catheter; End-stage renal disease in children; Renal replacement therapy.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval and informed consent
The national legislation with regard to ethics committee approval and patient informed consent was followed for all national registries providing data to the ESPN/ERA-EDTA Registry.
Figures
References
-
- European best practice guidelines for renal transplantation. Section IV Long-term management of the transplant recipient. IV.11 Paediatrics (specific problems) Nephrol Dial Transplant. 2002;17(Suppl 4):55–58. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
