

Pretransplant sequential hypo- and normothermic machine perfusion of suboptimal livers donated after circulatory death using a hemoglobin-based oxygen carrier perfusion solution
- PMID: 30588774
- PMCID: PMC6590255
- DOI: 10.1111/ajt.15228
Pretransplant sequential hypo- and normothermic machine perfusion of suboptimal livers donated after circulatory death using a hemoglobin-based oxygen carrier perfusion solution
Abstract
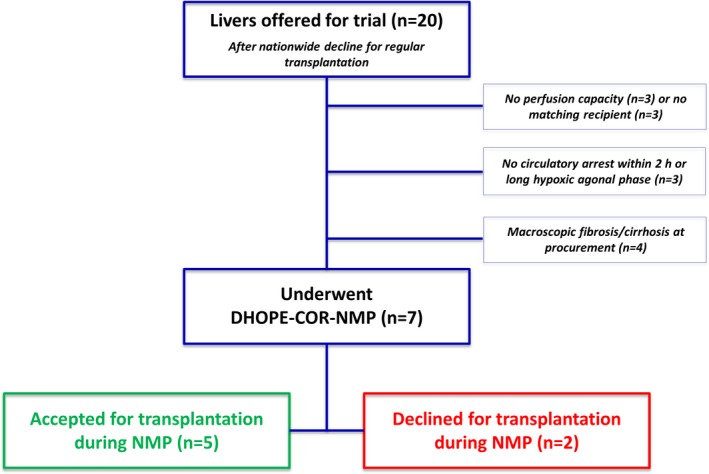
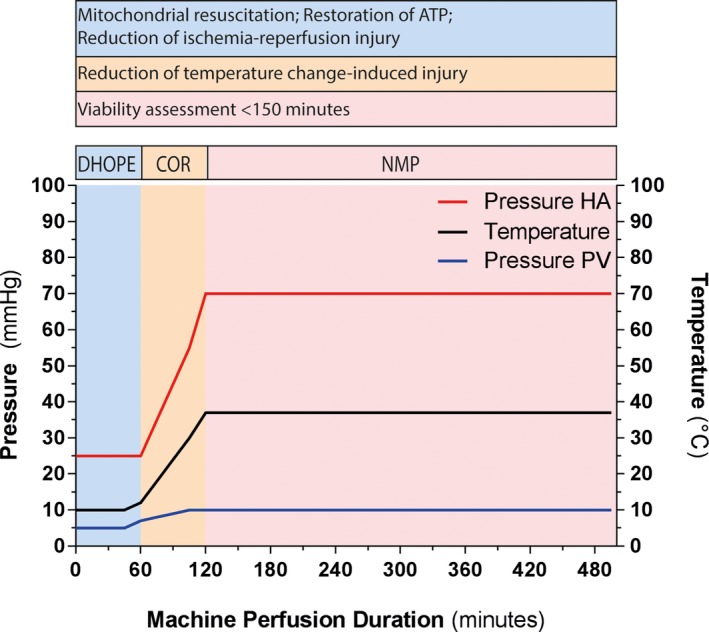
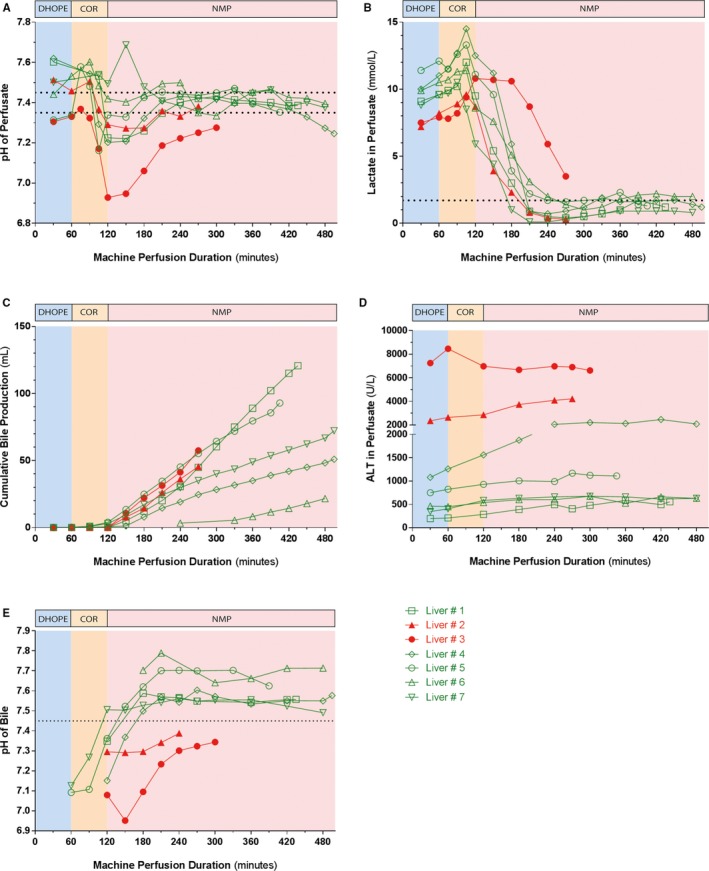
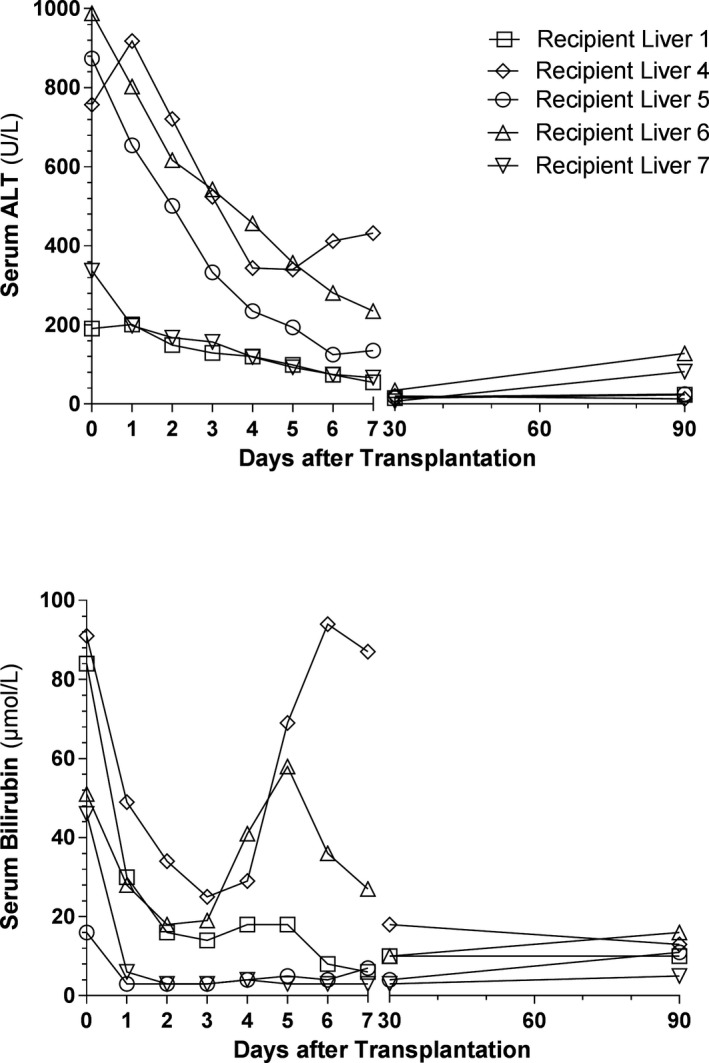
Ex situ dual hypothermic oxygenated machine perfusion (DHOPE) and normothermic machine perfusion (NMP) of donor livers may have a complementary effect when applied sequentially. While DHOPE resuscitates the mitochondria and increases hepatic adenosine triphosphate (ATP) content, NMP enables hepatobiliary viability assessment prior to transplantation. In contrast to DHOPE, NMP requires a perfusion solution with an oxygen carrier, for which red blood cells (RBC) have been used in most series. RBC, however, have limitations and cannot be used cold. We, therefore, established a protocol of sequential DHOPE, controlled oxygenated rewarming (COR), and NMP using a new hemoglobin-based oxygen carrier (HBOC)-based perfusion fluid (DHOPE-COR-NMP trial, NTR5972). Seven livers from donation after circulatory death (DCD) donors, which were initially declined for transplantation nationwide, underwent DHOPE-COR-NMP. Livers were considered transplantable if perfusate pH and lactate normalized, bile production was ≥10 mL and biliary pH > 7.45 within 150 minutes of NMP. Based on these criteria five livers were transplanted. The primary endpoint, 3-month graft survival, was a 100%. In conclusion, sequential DHOPE-COR-NMP using an HBOC-based perfusion fluid offers a novel method of liver machine perfusion for combined resuscitation and viability testing of suboptimal livers prior to transplantation.
Keywords: clinical research/practice; donors and donation: extended criteria; ischemia reperfusion injury (IRI); liver allograft function/dysfunction; liver transplantation/hepatology; organ perfusion and preservation; organ procurement; organ procurement and allocation.
© 2018 The Authors American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Dutkowski P, Polak WG, Muiesan P, et al. First comparison of hypothermic oxygenated PErfusion versus static cold storage of human donation after cardiac death liver transplants: an international‐matched case analysis. Ann Surg. 2015;262(5):1. - PubMed
-
- Perera T, Mergental H, Stephenson B, et al. First human liver transplantation using a marginal allograft resuscitated by normothermic machine perfusion. Liver Transpl. 2016;22(1):120‐124. - PubMed
-
- Watson CJ, Kosmoliaptsis V, Randle LV, et al. Preimplant normothermic liver perfusion of a suboptimal liver donated after circulatory death. Am J Transplant. 2016;16(1):353‐357. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
