

Analysis of the Prevalence of Microsatellite Instability in Prostate Cancer and Response to Immune Checkpoint Blockade
- PMID: 30589920
- PMCID: PMC6459218
- DOI: 10.1001/jamaoncol.2018.5801
Analysis of the Prevalence of Microsatellite Instability in Prostate Cancer and Response to Immune Checkpoint Blockade
Abstract
Importance: The anti-programmed cell death protein 1 (PD-1) antibody pembrolizumab is approved by the US Food and Drug Administration for the treatment of microsatellite instability-high (MSI-H) or mismatch repair-deficient (dMMR) solid tumors, but the prevalence of MSI-H/dMMR prostate cancer and the clinical utility of immune checkpoint blockade in this disease subset are unknown.
Objective: To define the prevalence of MSI-H/dMMR prostate cancer and the clinical benefit of anti-PD-1/programmed cell death 1 ligand 1 (PD-L1) therapy in this molecularly defined population.
Design, setting, and participants: In this case series, 1551 tumors from 1346 patients with prostate cancer undergoing treatment at Memorial Sloan Kettering Cancer Center were prospectively analyzed using a targeted sequencing assay from January 1, 2015, through January 31, 2018. Patients had a diagnosis of prostate cancer and consented to tumor molecular profiling when a tumor biopsy was planned or archival tissue was available. For each patient, clinical outcomes were reported, with follow-up until May 31, 2018.
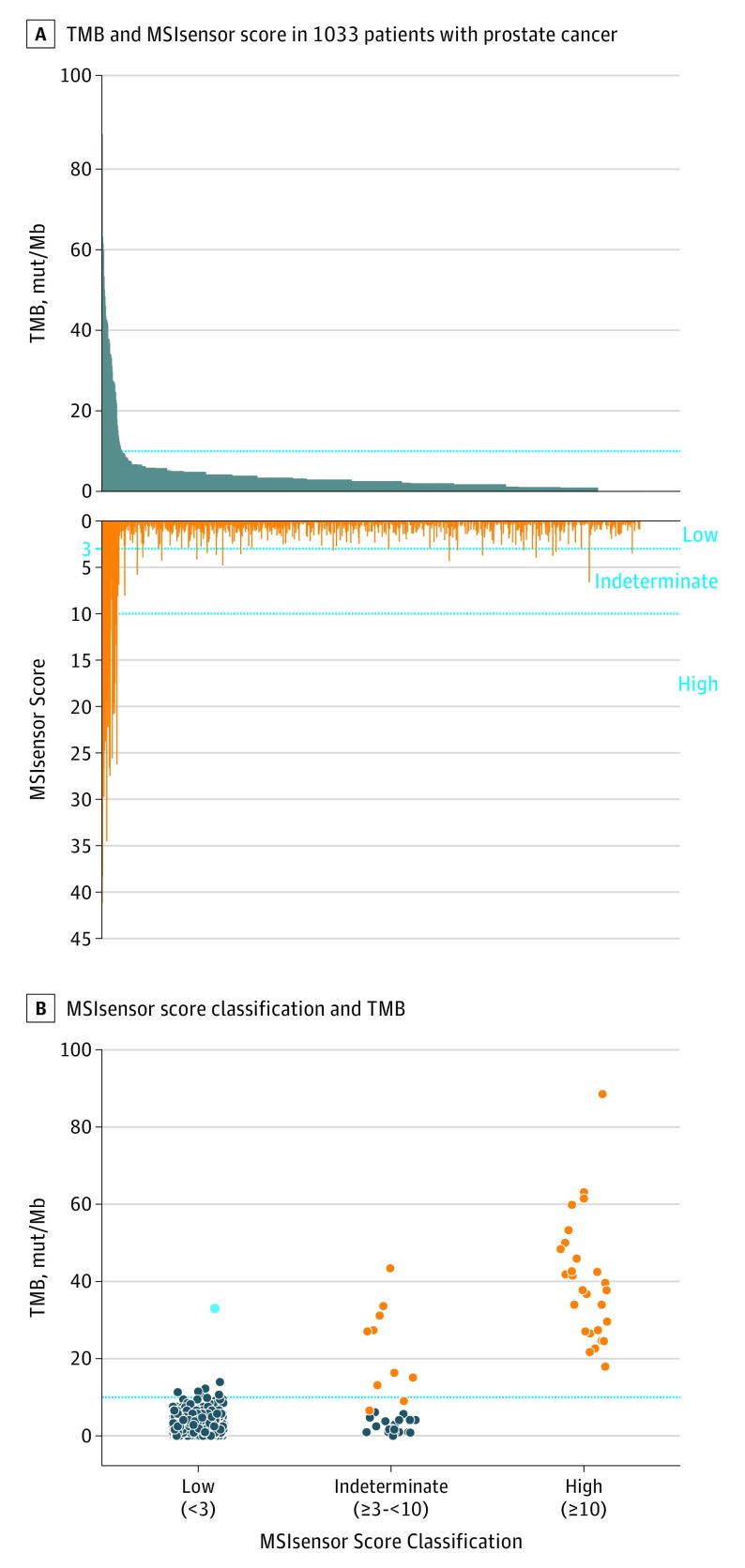
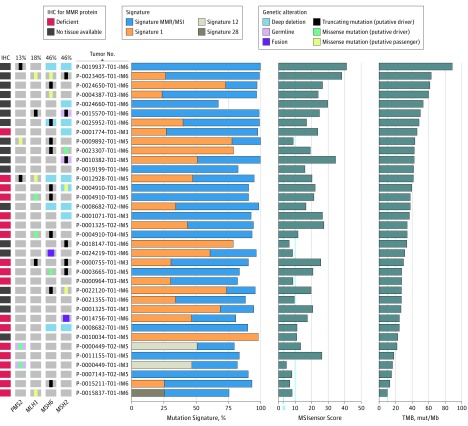
Main outcomes and measures: Tumor mutation burden and MSIsensor score, a quantitative measure of MSI, were calculated. Mutational signature analysis and immunohistochemistry for MMR protein expression were performed in select cases.
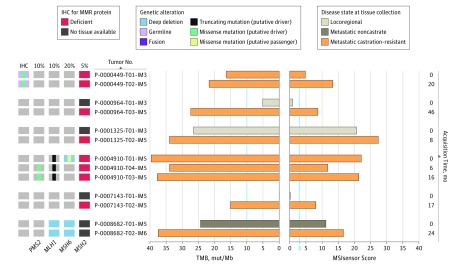
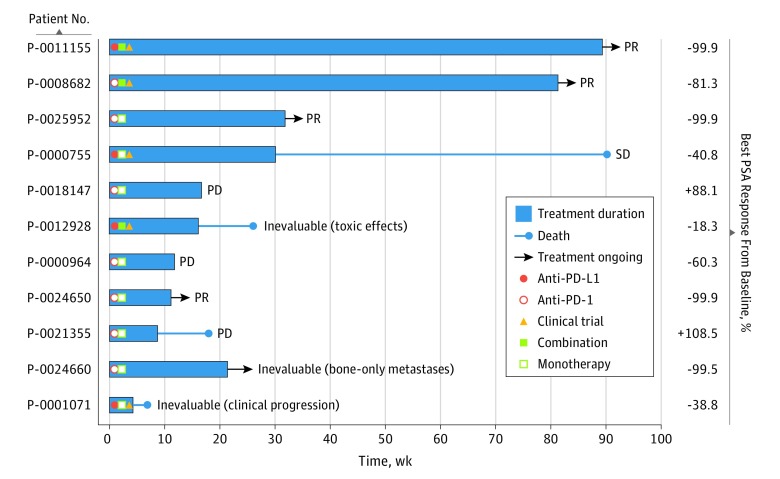
Results: Among the 1033 patients who had adequate tumor quality for MSIsensor analysis (mean [SD] age, 65.6 [9.3] years), 32 (3.1%) had MSI-H/dMMR prostate cancer. Twenty-three of 1033 patients (2.2%) had tumors with high MSIsensor scores, and an additional 9 had indeterminate scores with evidence of dMMR. Seven of the 32 MSI-H/dMMR patients (21.9%) had a pathogenic germline mutation in a Lynch syndrome-associated gene. Six patients had more than 1 tumor analyzed, 2 of whom displayed an acquired MSI-H phenotype later in their disease course. Eleven patients with MSI-H/dMMR castration-resistant prostate cancer received anti-PD-1/PD-L1 therapy. Six of these (54.5%) had a greater than 50% decline in prostate-specific antigen levels, 4 of whom had radiographic responses. As of May 2018, 5 of the 6 responders (5 of 11 total [45.5%]) were still on therapy for as long as 89 weeks.
Conclusions and relevance: The MSI-H/dMMR molecular phenotype is uncommon yet therapeutically meaningful in prostate cancer and can be somatically acquired during disease evolution. Given the potential for durable responses to anti-PD-1/PD-L1 therapy, these findings support the use of prospective tumor sequencing to screen all patients with advanced prostate cancer for MSI-H/dMMR. Because not all patients with the MSI-H/dMMR phenotype respond, further studies should explore mechanisms of resistance.
Conflict of interest statement
Figures
Comment in
-
Microsatellite Instability as an Emerging Biomarker for Checkpoint Inhibitor Response in Advanced Prostate Cancer.JAMA Oncol. 2019 Apr 1;5(4):478-479. doi: 10.1001/jamaoncol.2018.5789. JAMA Oncol. 2019. PMID: 30589921 No abstract available.
References
-
- Beer TM, Kwon ED, Drake CG, et al. Randomized, double-blind, phase III trial of ipilimumab versus placebo in asymptomatic or minimally symptomatic patients with metastatic chemotherapy-naive castration-resistant prostate cancer. J Clin Oncol. 2017;35(1):40-47. doi: 10.1200/JCO.2016.69.1584 - DOI - PubMed
-
- Kwon ED, Drake CG, Scher HI, et al. ; CA184-043 Investigators . Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(7):700-712. doi: 10.1016/S1470-2045(14)70189-5 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
