

An expandable approach for design and personalization of digital, just-in-time adaptive interventions
- PMID: 30590757
- PMCID: PMC6351973
- DOI: 10.1093/jamia/ocy160
An expandable approach for design and personalization of digital, just-in-time adaptive interventions
Abstract
Objective: We aim to deliver a framework with 2 main objectives: 1) facilitating the design of theory-driven, adaptive, digital interventions addressing chronic illnesses or health problems and 2) producing personalized intervention delivery strategies to support self-management by optimizing various intervention components tailored to people's individual needs, momentary contexts, and psychosocial variables.
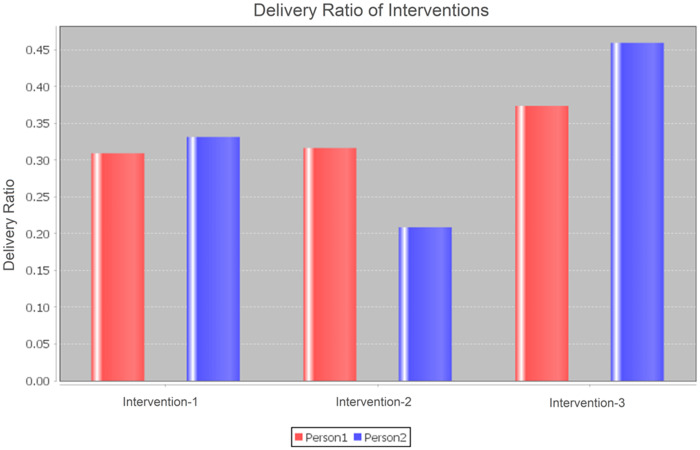
Materials and methods: We propose a template-based digital intervention design mechanism enabling the configuration of evidence-based, just-in-time, adaptive intervention components. The design mechanism incorporates a rule definition language enabling experts to specify triggering conditions for interventions based on momentary and historical contextual/personal data. The framework continuously monitors and processes personal data space and evaluates intervention-triggering conditions. We benefit from reinforcement learning methods to develop personalized intervention delivery strategies with respect to timing, frequency, and type (content) of interventions. To validate the personalization algorithm, we lay out a simulation testbed with 2 personas, differing in their various simulated real-life conditions.
Results: We evaluate the design mechanism by presenting example intervention definitions based on behavior change taxonomies and clinical guidelines. Furthermore, we provide intervention definitions for a real-world care program targeting diabetes patients. Finally, we validate the personalized delivery mechanism through a set of hypotheses, asserting certain ways of adaptation in the delivery strategy, according to the differences in simulation related to personal preferences, traits, and lifestyle patterns.
Conclusion: While the design mechanism is sufficiently expandable to meet the theoretical and clinical intervention design requirements, the personalization algorithm is capable of adapting intervention delivery strategies for simulated real-life conditions.
Figures
Similar articles
-
A reinforcement learning based algorithm for personalization of digital, just-in-time, adaptive interventions.Artif Intell Med. 2021 May;115:102062. doi: 10.1016/j.artmed.2021.102062. Epub 2021 Apr 2. Artif Intell Med. 2021. PMID: 34001322
-
The potential of digital phenotyping to advance the contributions of mobile health to self-management science.Nurs Outlook. 2020 Sep-Oct;68(5):548-559. doi: 10.1016/j.outlook.2020.03.007. Epub 2020 May 8. Nurs Outlook. 2020. PMID: 32402392
-
Toward a Digital Platform for the Self-Management of Noncommunicable Disease: Systematic Review of Platform-Like Interventions.J Med Internet Res. 2020 Oct 28;22(10):e16774. doi: 10.2196/16774. J Med Internet Res. 2020. PMID: 33112239 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Helping patients help themselves: A systematic review of self-management support strategies in primary health care practice.PLoS One. 2019 Aug 1;14(8):e0220116. doi: 10.1371/journal.pone.0220116. eCollection 2019. PLoS One. 2019. PMID: 31369582 Free PMC article.
Cited by
-
The journey to transparency, reproducibility, and replicability.J Am Med Inform Assoc. 2019 Mar 1;26(3):185-187. doi: 10.1093/jamia/ocz007. J Am Med Inform Assoc. 2019. PMID: 30689885 Free PMC article. No abstract available.
-
Bayesian strategy selection identifies optimal solutions to complex problems using an example from GP prescribing.NPJ Digit Med. 2020 Jan 20;3:7. doi: 10.1038/s41746-019-0205-y. eCollection 2020. NPJ Digit Med. 2020. PMID: 31993505 Free PMC article.
-
Precision clinical trials: a framework for getting to precision medicine for neurobehavioural disorders.J Psychiatry Neurosci. 2021 Jan 4;46(1):E97-E110. doi: 10.1503/jpn.200042. J Psychiatry Neurosci. 2021. PMID: 33206039 Free PMC article. Review.
-
Digital headache self-management interventions for patients with a primary headache disorder: A systematic review of randomized controlled trials.Headache. 2022 Oct;62(9):1105-1119. doi: 10.1111/head.14392. Headache. 2022. PMID: 36286601 Free PMC article.
-
Key facets to build up eHealth and mHealth interventions to enhance physical activity, sedentary behavior and nutrition in healthy subjects - an umbrella review.BMC Public Health. 2020 Oct 23;20(1):1605. doi: 10.1186/s12889-020-09700-7. BMC Public Health. 2020. PMID: 33097013 Free PMC article.
References
-
- Spruijt-Metz D, Nilsen W.. Dynamic models of behavior for just-in-time adaptive interventions. IEEE Pervasive Comput 2014; 13 (3): 13–7.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
